Cressey Tim R, Punyawudho Baralee, Le Coeur Sophie, Jourdain Gonzague, Saenjum Chalermpong, Capparelli Edmund V, Jittayanun Kanokwan, Phanomcheong Siriluk, Luvira Anita, Borkird Thitiporn, Puangsombat Achara, Aarons Leon, Sukrakanchana Pra-Ornsuda, Urien Saik, Lallemant Marc
*PHPT/IRD 174, Faculty of Associated Medical Sciences, Chiang Mai University, Chiang Mai, Thailand; †Department of Immunology and Infectious Diseases, Harvard T.H Chan School of Public Health, Boston, MA; ‡Department of Molecular and Clinical Pharmacology, University of Liverpool, Liverpool, United Kingdom; §Department of Pharmaceutical Care, Faculty of Pharmacy, Chiang Mai University, Chiang Mai, Thailand; ‖Institut d'Etudes Démographiques, Paris, France; ¶Institut de Recherche pour le Développement (IRD) UMI 174-PHPT, Marseille, France; #Department of Pharmaceutical Sciences, Faculty of Pharmacy, Chiang Mai University, Chiang Mai, Thailand; **Skaggs School of Pharmacy and Pharmaceutical Sciences, University of California San Diego, La Jolla, CA; ††Department of Pediatric, Health Promotion Center Region 10, Chiang Mai, Thailand; ‡‡Department of Pediatric, Banglamung Hospital, Chonburi, Thailand; §§Department of Pediatric, Nopparat Rajathanee Hospital, Bangkok, Thailand; ‖‖Department of Pediatric, Hat Yai Hospital, Hat Yai, Thailand; ¶¶Department of Pediatric, Samutprakarn Hospital, Samut Prakan, Thailand; ##Manchester Pharmacy School, The University of Manchester, Manchester, United Kingdom; and ***EAU7323 Université Paris Descartes, Sorbonne Paris Cité, Paris, France.
J Acquir Immune Defic Syndr. 2017 Aug 15;75(5):554-560. doi: 10.1097/QAI.0000000000001447.
Nevirapine (NVP) is a key component of antiretroviral prophylaxis and treatment for neonates. We evaluated current World Health Organization (WHO) weight-band NVP prophylactic dosing recommendations and investigated optimal therapeutic NVP dosing for neonates.
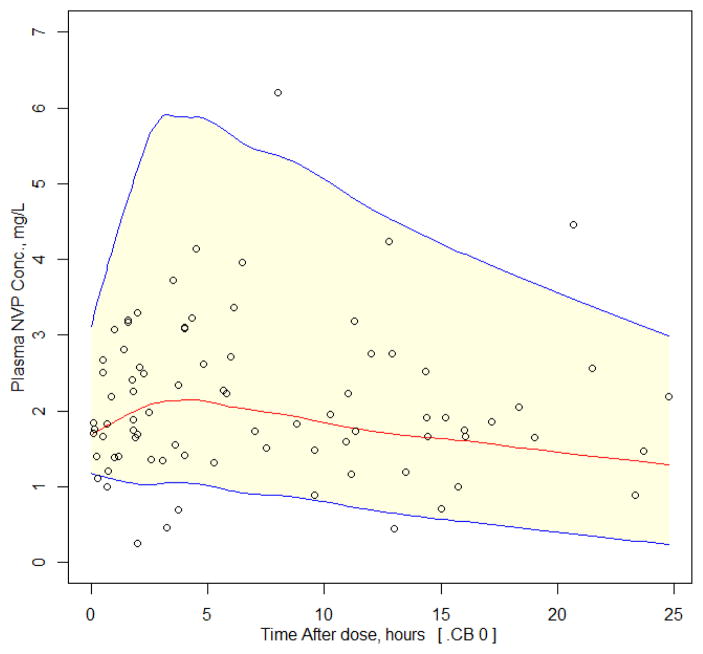
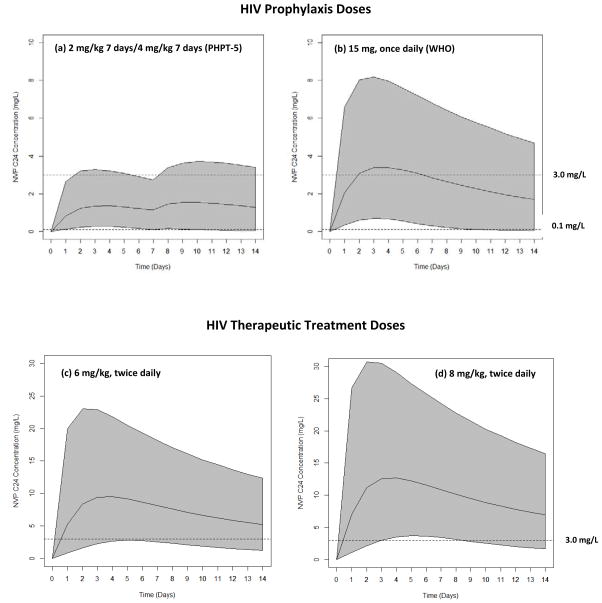
The PHPT-5 study in Thailand assessed the efficacy of "Perinatal Antiretroviral Intensification" to prevent mother-to-child transmission of HIV in women with <8 weeks of antiretroviral treatment before delivery (NCT01511237). Infants received a 2-week course of zidovudine/lamivudine/NVP (NVP syrup/once daily: 2 mg/kg for 7 days; then 4 mg/kg for 7 days). Infant samples were assessed during the first 2 weeks of life. NVP population pharmacokinetics (PK) parameters were estimated using nonlinear mixed-effects models. Simulations were performed to estimate the probability of achieving target NVP trough concentrations for prophylaxis (>0.10 mg/L) and for therapeutic efficacy (>3.0 mg/L) using different infant dosing strategies.
Sixty infants (55% male) were included. At birth, median (range) weight was 2.9 (2.3-3.6) kg. NVP concentrations were best described by a 1-compartment PK model. Infant weight and postnatal age influenced NVP PK parameters. Based on simulations for a 3-kg infant, ≥92% would have an NVP trough >0.1 mg/L after 48 hours through 2 weeks using the PHPT-5 and WHO-dosing regimens. For NVP-based therapy, a 6-mg/kg twice daily dose produced a trough >3.0 mg/L in 87% of infants at 48 hours and 80% at 2 weeks.
WHO weight-band prophylactic guidelines achieved target concentrations. Starting NVP 6 mg/kg twice daily from birth is expected to achieve therapeutic concentrations during the first 2 weeks of life.
奈韦拉平(NVP)是新生儿抗逆转录病毒预防和治疗的关键组成部分。我们评估了世界卫生组织(WHO)当前的体重范围NVP预防性给药建议,并研究了新生儿的最佳治疗性NVP给药方案。
泰国的PHPT - 5研究评估了“围产期抗逆转录病毒强化治疗”对分娩前接受抗逆转录病毒治疗少于8周的女性预防母婴传播HIV的疗效(NCT01511237)。婴儿接受为期2周的齐多夫定/拉米夫定/NVP疗程(NVP糖浆/每日一次:2mg/kg,共7天;然后4mg/kg,共7天)。在婴儿出生后的前2周对样本进行评估。使用非线性混合效应模型估计NVP群体药代动力学(PK)参数。进行模拟以估计使用不同婴儿给药策略达到预防目标NVP谷浓度(>0.10mg/L)和治疗效果目标NVP谷浓度(>3.0mg/L)的概率。
纳入了60名婴儿(55%为男性)。出生时,体重中位数(范围)为2.9(2.3 - 3.6)kg。NVP浓度最好用单室PK模型描述。婴儿体重和出生后年龄影响NVP PK参数。基于对一名3kg婴儿的模拟,使用PHPT - 5和WHO给药方案,≥92%的婴儿在48小时至2周后NVP谷浓度>0.1mg/L。对于基于NVP的治疗,每日两次6mg/kg的剂量在48小时时使87%的婴儿谷浓度>3.0mg/L,在2周时使80%的婴儿谷浓度>3.0mg/L。
WHO体重范围预防性指南达到了目标浓度。从出生开始每日两次给予6mg/kg的NVP预计在出生后的前2周达到治疗浓度。