Troisi Jacopo, Pierri Luca, Landolfi Annamaria, Marciano Francesca, Bisogno Antonella, Belmonte Federica, Palladino Carmen, Guercio Nuzio Salvatore, Campiglia Pietro, Vajro Pietro
Department of Medicine, Surgery and Dentistry "Scuola Medica Salernitana", Pediatric Section, University of Salerno, Via S. Allende, 84081 Baronissi (SA), Italy.
Theoreo srl, Via degli Ulivi 3, 84090 Montecorvino Pugliano (SA), Italy.
Nutrients. 2017 May 11;9(5):485. doi: 10.3390/nu9050485.
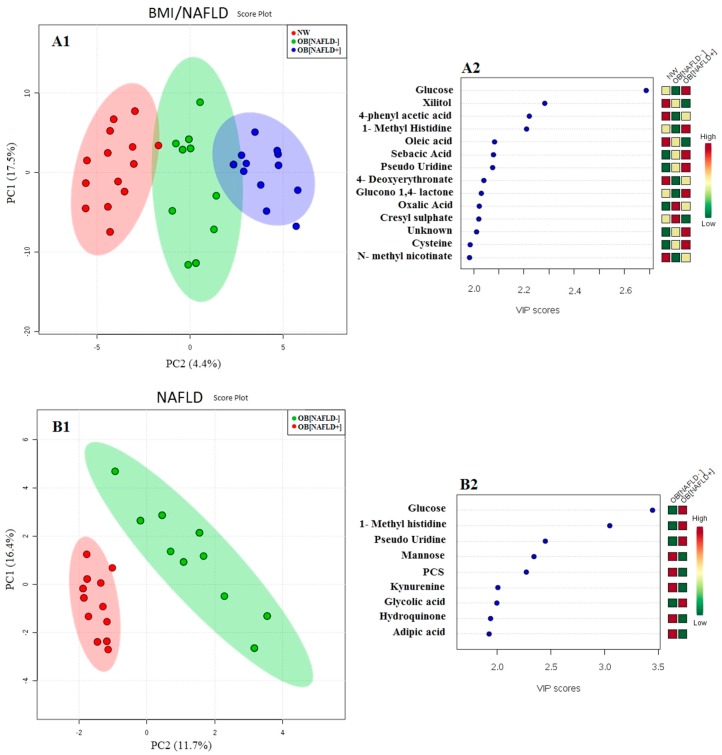
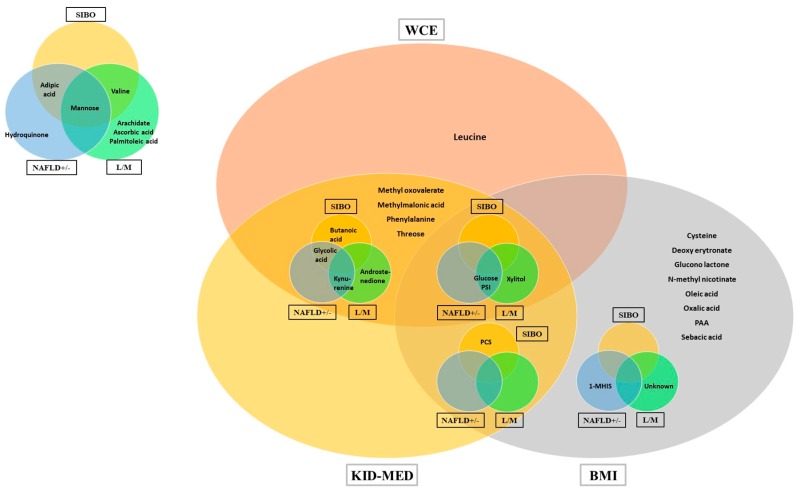
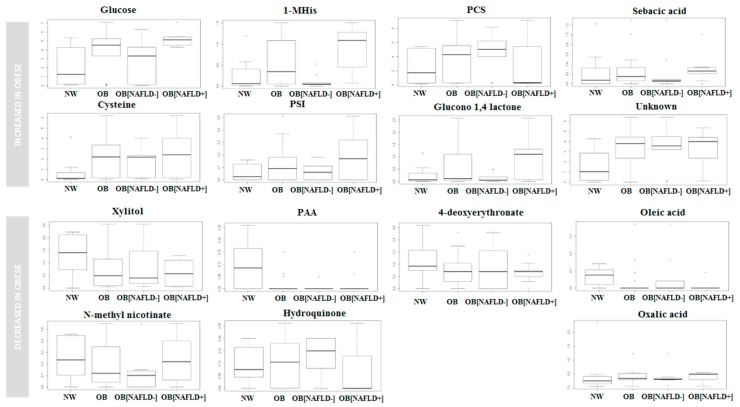
To get insight into still elusive pathomechanisms of pediatric obesity and non-alcoholic fatty liver disease (NAFLD) we explored the interplay among GC-MS studied urinary metabolomic signature, gut liver axis (GLA) abnormalities, and food preferences (Kid-Med). Intestinal permeability (IP), small intestinal bacterial overgrowth (SIBO), and homeostatic model assessment-insulin resistance were investigated in forty children (mean age 9.8 years) categorized as normal weight (NW) or obese (body mass index <85th or >95th percentile, respectively) ± ultrasonographic bright liver and hypertransaminasemia (NAFLD). SIBO was increased in all obese children ( 0.0022), IP preferentially in those with NAFLD ( 0.0002). The partial least-square discriminant analysis of urinary metabolome correctly allocated children based on their obesity, NAFLD, visceral fat, pathological IP and SIBO. Compared to NW, obese children had (1) higher levels of glucose/1-methylhistidine, the latter more markedly in NAFLD patients; and (2) lower levels of xylitol, phenyl acetic acid and hydroquinone, the latter especially in children without NAFLD. The metabolic pathways of BCAA and/or their metabolites correlated with excess of visceral fat centimeters (leucine/oxo-valerate), and more deranged IP and SIBO (valine metabolites). Urinary metabolome analysis contributes to define a metabolic fingerprint of pediatric obesity and related NAFLD, by identifying metabolic pathways/metabolites reflecting typical obesity dietary habits and GLA perturbations.
为深入了解儿童肥胖和非酒精性脂肪性肝病(NAFLD)仍难以捉摸的发病机制,我们探讨了气相色谱 - 质谱联用(GC - MS)研究的尿液代谢组学特征、肠肝轴(GLA)异常和食物偏好(儿童医学问卷)之间的相互作用。对40名儿童(平均年龄9.8岁)进行了肠道通透性(IP)、小肠细菌过度生长(SIBO)和稳态模型评估 - 胰岛素抵抗的研究,这些儿童被分类为正常体重(NW)或肥胖(体重指数分别<第85百分位数或>第95百分位数)±超声检查肝脏回声增强和转氨酶升高(NAFLD)。所有肥胖儿童的SIBO均增加(P = 0.0022),IP在患有NAFLD的儿童中更常见(P = 0.0002)。尿液代谢组的偏最小二乘判别分析能够根据儿童的肥胖、NAFLD、内脏脂肪、病理性IP和SIBO正确分类。与NW儿童相比,肥胖儿童有:(1)葡萄糖/1 - 甲基组氨酸水平较高,在NAFLD患者中更为明显;(2)木糖醇、苯乙酸和对苯二酚水平较低,后者在无NAFLD的儿童中尤为明显。支链氨基酸(BCAA)和/或其代谢产物的代谢途径与内脏脂肪厘米数过多(亮氨酸/氧代戊酸)以及更紊乱的IP和SIBO(缬氨酸代谢产物)相关。尿液代谢组分析通过识别反映典型肥胖饮食习惯和GLA紊乱的代谢途径/代谢产物,有助于定义儿童肥胖和相关NAFLD的代谢指纹。