Zhang Xuanping, Devlin Heather M, Smith Bryce, Imperatore Giuseppina, Thomas William, Lobelo Felipe, Ali Mohammed K, Norris Keri, Gruss Stephanie, Bardenheier Barbara, Cho Pyone, Garcia de Quevedo Isabel, Mudaliar Uma, Jones Christopher D, Durthaler Jeffrey M, Saaddine Jinan, Geiss Linda S, Gregg Edward W
Division of Diabetes Translation, National Centers for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, Atlanta, Georgia, United States of America.
Office of Public Health Scientific Services, Centers for Disease Control and Prevention, Atlanta, Georgia, United States of America.
PLoS One. 2017 May 11;12(5):e0176436. doi: 10.1371/journal.pone.0176436. eCollection 2017.
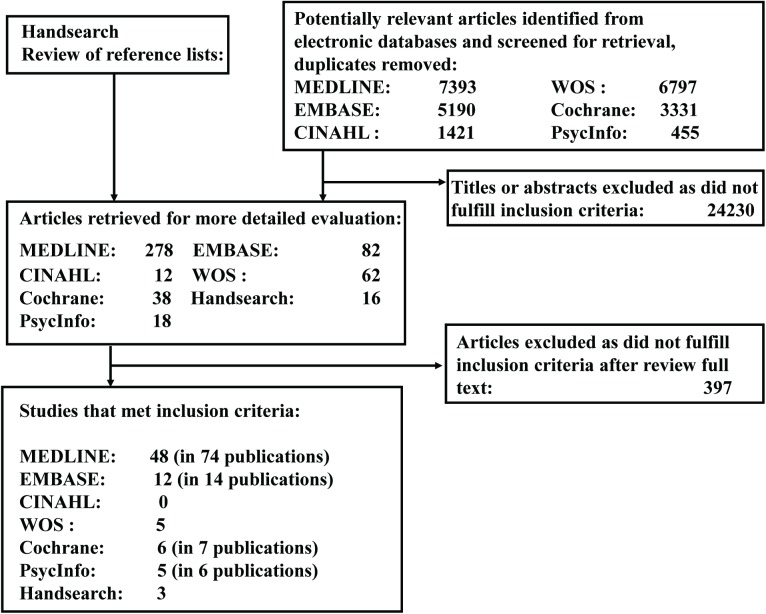
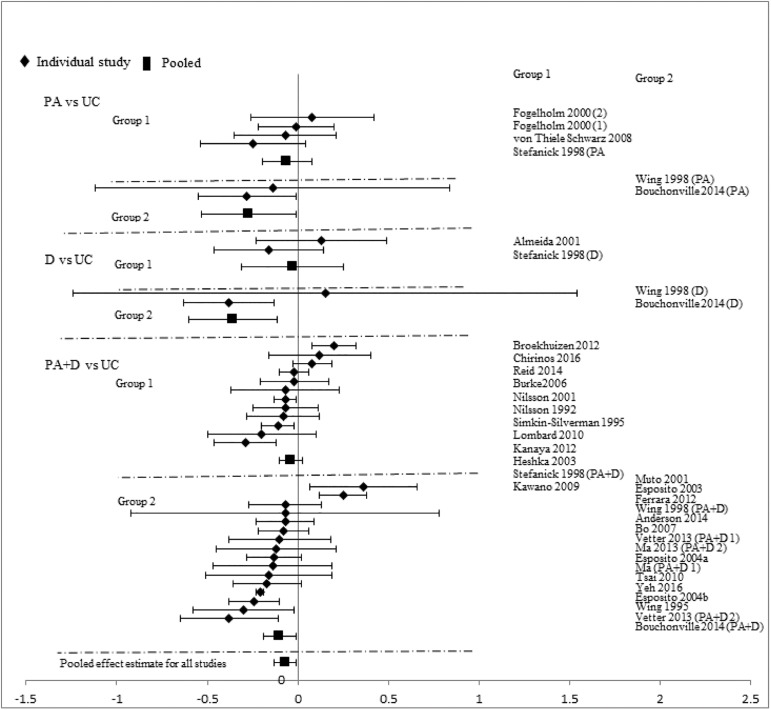
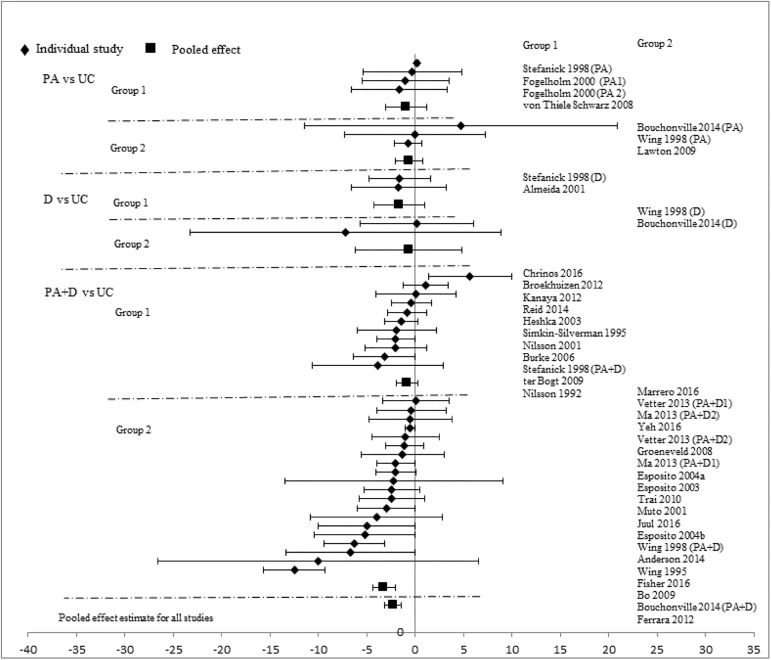
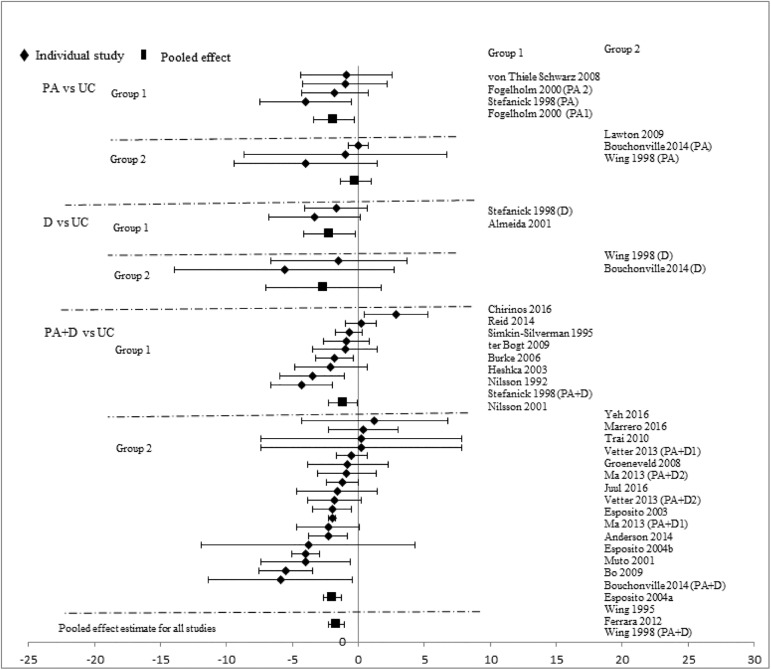
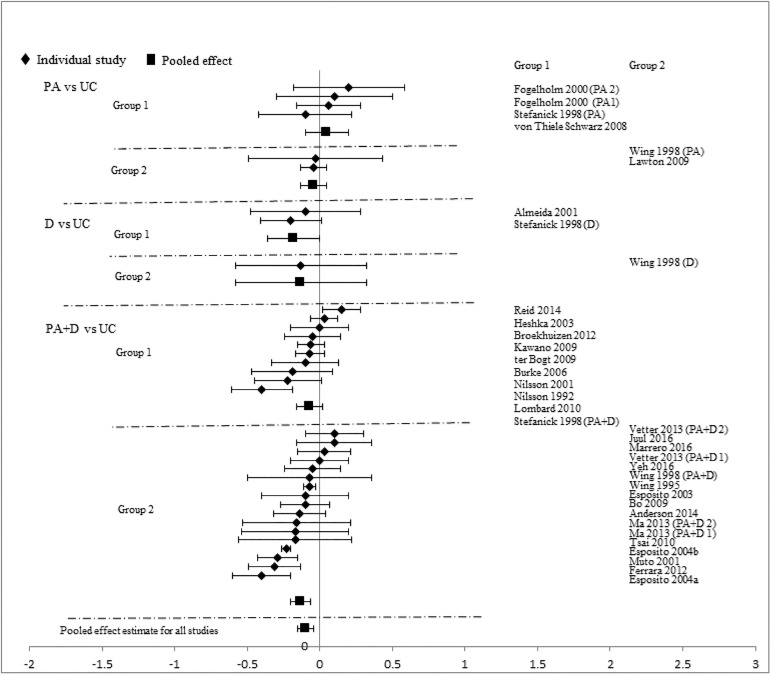
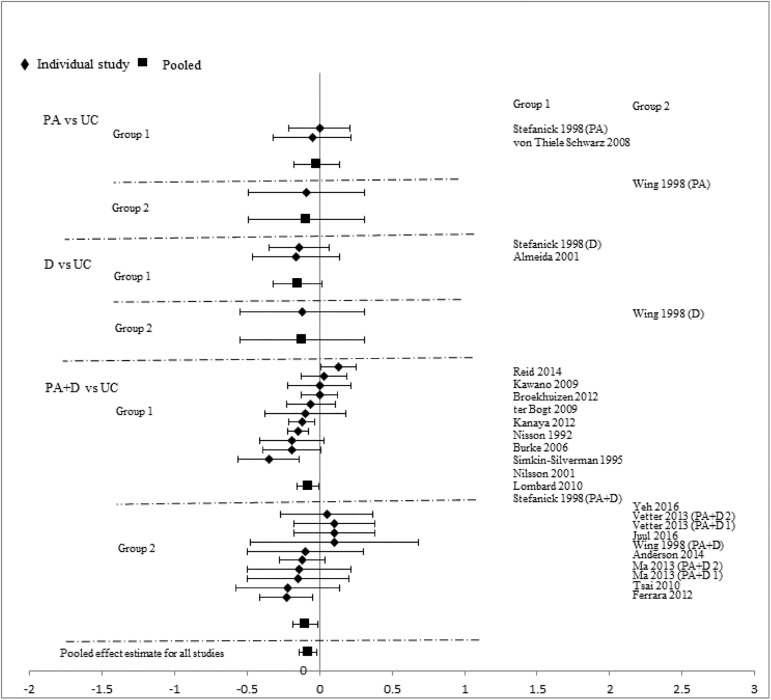
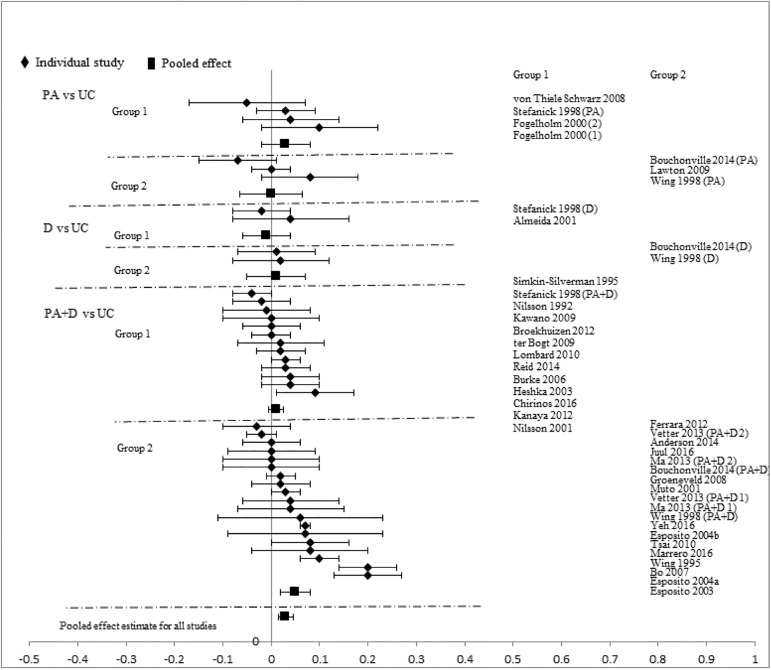
Structured lifestyle interventions can reduce diabetes incidence and cardiovascular disease (CVD) risk among persons with impaired glucose tolerance (IGT), but it is unclear whether they should be implemented among persons without IGT. We conducted a systematic review and meta-analyses to assess the effectiveness of lifestyle interventions on CVD risk among adults without IGT or diabetes. We systematically searched MEDLINE, EMBASE, CINAHL, Web of Science, the Cochrane Library, and PsychInfo databases, from inception to May 4, 2016. We selected randomized controlled trials of lifestyle interventions, involving physical activity (PA), dietary (D), or combined strategies (PA+D) with follow-up duration ≥12 months. We excluded all studies that included individuals with IGT, confirmed by 2-hours oral glucose tolerance test (75g), but included all other studies recruiting populations with different glycemic levels. We stratified studies by baseline glycemic levels: (1) low-range group with mean fasting plasma glucose (FPG) <5.5mmol/L or glycated hemoglobin (A1C) <5.5%, and (2) high-range group with FPG ≥5.5mmol/L or A1C ≥5.5%, and synthesized data using random-effects models. Primary outcomes in this review included systolic blood pressure (SBP), diastolic blood pressure (DBP), total cholesterol (TC), low density lipoprotein cholesterol (LDL-C), high density lipoprotein cholesterol (HDL-C), and triglycerides (TG). Totally 79 studies met inclusion criteria. Compared to usual care (UC), lifestyle interventions achieved significant improvements in SBP (-2.16mmHg[95%CI, -2.93, -1.39]), DBP (-1.83mmHg[-2.34, -1.31]), TC (-0.10mmol/L[-0.15, -0.05]), LDL-C (-0.09mmol/L[-0.13, -0.04]), HDL-C (0.03mmol/L[0.01, 0.04]), and TG (-0.08mmol/L[-0.14, -0.03]). Similar effects were observed among both low-and high-range study groups except for TC and TG. Similar effects also appeared in SBP and DBP categories regardless of follow-up duration. PA+D interventions had larger improvement effects on CVD risk factors than PA alone interventions. In adults without IGT or diabetes, lifestyle interventions resulted in significant improvements in SBP, DBP, TC, LDL-C, HDL-C, and TG, and might further reduce CVD risk.
结构化生活方式干预可降低糖耐量受损(IGT)人群的糖尿病发病率和心血管疾病(CVD)风险,但对于无IGT的人群是否应实施此类干预尚不清楚。我们进行了一项系统评价和荟萃分析,以评估生活方式干预对无IGT或糖尿病的成年人CVD风险的有效性。我们系统检索了MEDLINE、EMBASE、CINAHL、Web of Science、Cochrane图书馆和PsychInfo数据库,检索时间从建库至2016年5月4日。我们选择了生活方式干预的随机对照试验,包括体育活动(PA)、饮食(D)或联合策略(PA+D),随访时间≥12个月。我们排除了所有经2小时口服葡萄糖耐量试验(75g)确诊有IGT个体的研究,但纳入了所有其他招募不同血糖水平人群的研究。我们根据基线血糖水平对研究进行分层:(1)低范围组,平均空腹血糖(FPG)<5.5mmol/L或糖化血红蛋白(A1C)<5.5%;(2)高范围组,FPG≥5.5mmol/L或A1C≥5.5%,并使用随机效应模型合成数据。本评价的主要结局包括收缩压(SBP)、舒张压(DBP)、总胆固醇(TC)、低密度脂蛋白胆固醇(LDL-C)、高密度脂蛋白胆固醇(HDL-C)和甘油三酯(TG)。共有79项研究符合纳入标准。与常规护理(UC)相比,生活方式干预在SBP(-2.16mmHg[95%CI,-2.93,-1.39])、DBP(-1.83mmHg[-2.3, -1.31])、TC(-0.10mmol/L[-0.15, -0.05])、LDL-C(-0.09mmol/L[-0.13, -0.04])、HDL-C(0.03mmol/L[0.01, 0.04])和TG(-0.08mmol/L[-0.14, -0.03])方面有显著改善。除TC和TG外,在低范围和高范围研究组中均观察到类似效果。无论随访时间长短,SBP和DBP类别中也出现了类似效果。PA+D干预对CVD危险因素的改善作用大于单独的PA干预。在无IGT或糖尿病的成年人中,生活方式干预使SBP、DBP、TC、LDL-C、HDL-C和TG有显著改善,并可能进一步降低CVD风险。