Hawkes Sarah, Buse Kent, Kapilashrami Anuj
Institute for Global Health, University College London, 30, Guilford Street, London, WC1N 1EH, UK.
UNAIDS, Geneva, Switzerland.
Global Health. 2017 May 12;13(1):26. doi: 10.1186/s12992-017-0249-1.
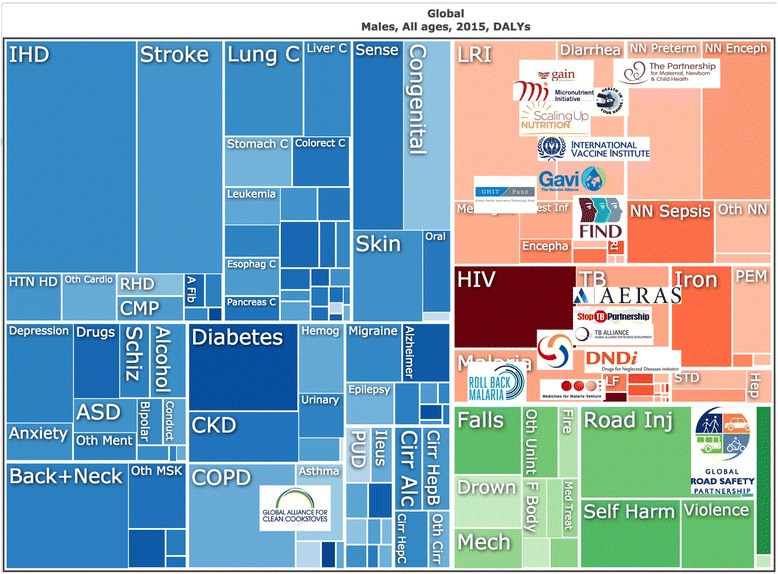
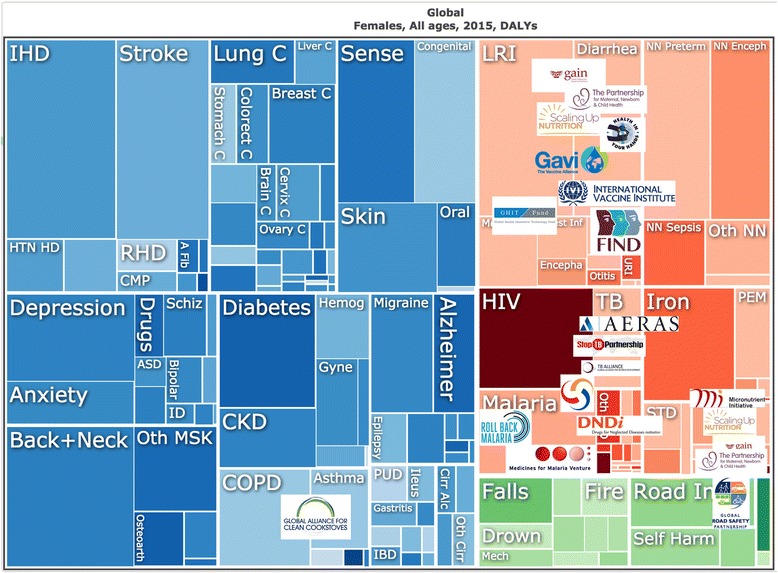
The Global Public Private Partnerships for Health (GPPPH) constitute an increasingly central part of the global health architecture and carry both financial and normative power. Gender is an important determinant of health status, influencing differences in exposure to health determinants, health behaviours, and the response of the health system. We identified 18 GPPPH - defined as global institutions with a formal governance mechanism which includes both public and private for-profit sector actors - and conducted a gender analysis of each.
Gender was poorly mainstreamed through the institutional functioning of the partnerships. Half of these partnerships had no mention of gender in their overall institutional strategy and only three partnerships had a specific gender strategy. Fifteen governing bodies had more men than women - up to a ratio of 5:1. Very few partnerships reported sex-disaggregated data in their annual reports or coverage/impact results. The majority of partnerships focused their work on maternal and child health and infectious and communicable diseases - none addressed non-communicable diseases (NCDs) directly, despite the strong role that gender plays in determining risk for the major NCD burdens.
We propose two areas of action in response to these findings. First, GPPPH need to become serious in how they "do" gender; it needs to be mainstreamed through the regular activities, deliverables and systems of accountability. Second, the entire global health community needs to pay greater attention to tackling the major burden of NCDs, including addressing the gendered nature of risk. Given the inherent conflicts of interest in tackling the determinants of many NCDs, it is debatable whether the emergent GPPPH model will be an appropriate one for addressing NCDs.
全球卫生公私伙伴关系(GPPPH)在全球卫生架构中日益占据核心地位,兼具财政和规范影响力。性别是健康状况的重要决定因素,影响着人们接触健康决定因素、健康行为以及卫生系统反应方面的差异。我们确定了18个GPPPH(定义为具有正式治理机制的全球机构,其中包括公共和私营营利部门行为体),并对每个机构进行了性别分析。
通过伙伴关系的机构运作,性别平等未得到充分主流化。这些伙伴关系中有一半在其整体机构战略中未提及性别,只有三个伙伴关系有具体的性别战略。15个理事机构中男性多于女性,比例高达5:1。很少有伙伴关系在其年度报告或覆盖范围/影响结果中报告按性别分类的数据。大多数伙伴关系将工作重点放在孕产妇和儿童健康以及传染病上,尽管性别在决定主要非传染性疾病负担风险方面发挥着重要作用,但没有一个直接涉及非传染性疾病(NCDs)。
针对这些发现,我们提出两个行动领域。首先,GPPPH需要认真对待其如何“落实”性别平等问题;需要通过常规活动、可交付成果和问责制度将其主流化。其次,整个全球卫生界需要更加关注应对非传染性疾病的主要负担,包括解决风险的性别特征问题。鉴于在应对许多非传染性疾病决定因素方面存在内在利益冲突,新兴的GPPPH模式是否适合应对非传染性疾病值得商榷。