Nieder Carsten, Tollali Terje, Yobuta Rosalba, Reigstad Anne, Flatoy Liv Randi, Pawinski Adam
Department of Oncology and Palliative Medicine, Nordland Hospital Trust, Bodo, Norway.
Department of Clinical Medicine, Faculty of Health Sciences, University of Tromso, Tromso, Norway.
J Clin Med Res. 2017 Jun;9(6):482-487. doi: 10.14740/jocmr2980w. Epub 2017 Apr 26.
Effective symptom palliation can be achieved with low-dose palliative thoracic radiotherapy. In several studies, median survival was not improved with higher doses of radiation. More controversy exists regarding the impact of higher doses on 1- and 2-year survival rates. Therefore, a comparison of survival outcomes after radiotherapy with different biologically equivalent doses (equivalent dose in 2-Gy fractions, EQD2) was performed.
This was a retrospective single-institution study of 232 patients with small or non-small cell lung cancer. Most commonly 2 fractions of 8.5 Gy were prescribed (34%), followed by 10 fractions of 3 Gy or equivalent regimens (30%, EQD2 circa 33 Gy). The highest EQD2 consisted of 45 Gy. Intention-to-treat analyses were performed.
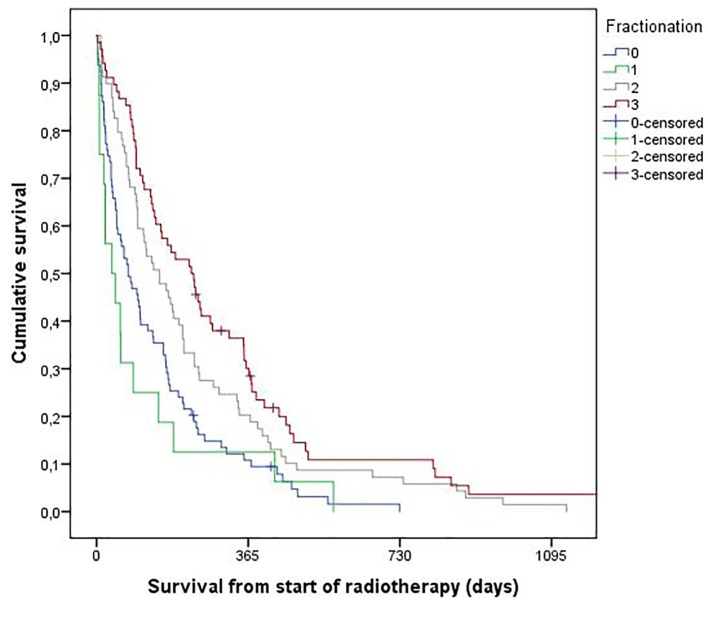
Survival was significantly shorter with regimens of intended EQD2 < 33 Gy, e.g., 2 fractions of 8.5 Gy (median 2.5 months compared to 5.0 and 7.5 months with EQD2 of circa 33 and 45 Gy, respectively). The 2-year survival rates were 0%, 7% and 11%, respectively. In 128 prognostically favorable patients, median survival was comparable for the three different dose levels (6 - 8.3 months). The 2-year survival rates were 0%, 10%, and 13%, respectively (not statistically significant).
Although most of the observed survival differences diminished after exclusion of poor prognosis patients with reduced performance status and/or progressive extrathoracic disease, a slight increase in 2-year survival rates with higher EQD2 cannot be excluded. Because of relatively small improvements, a confirmatory randomized trial in this subgroup would have to include a large number of patients.
低剂量姑息性胸部放疗可有效缓解症状。在多项研究中,更高剂量的放疗并未改善中位生存期。关于更高剂量对1年和2年生存率的影响存在更多争议。因此,对不同生物等效剂量(2 Gy分割剂量下的等效剂量,EQD2)放疗后的生存结果进行了比较。
这是一项对232例小细胞或非小细胞肺癌患者的单机构回顾性研究。最常用的处方是2次分割,每次8.5 Gy(34%),其次是10次分割,每次3 Gy或等效方案(30%,EQD2约为33 Gy)。最高的EQD2为45 Gy。进行了意向性分析。
预期EQD2 < 33 Gy的方案生存率显著缩短,例如2次分割,每次8.5 Gy(中位生存期为2.5个月,而EQD2约为33 Gy和45 Gy时分别为5.0个月和7.5个月)。2年生存率分别为0%、7%和11%。在128例预后良好的患者中,三种不同剂量水平的中位生存期相当(6 - 8.3个月)。2年生存率分别为0%、10%和13%(无统计学意义)。
尽管在排除了身体状况下降和/或胸外疾病进展的预后不良患者后,观察到的大多数生存差异有所减小,但不能排除EQD2较高时2年生存率略有增加的情况。由于改善相对较小,在该亚组中进行的验证性随机试验将不得不纳入大量患者。