Landeweer Elleke, Molewijk Bert, Hem Marit Helene, Pedersen Reidar
Center for Medical Ethics, Institute of Health and Society, Faculty of Medicine, University of Oslo, P.O. Box 1130, Blindern, Oslo, NO, 0318, Norway.
Department of Medical Humanities, VU University Medical Center, Amsterdam, The Netherlands.
BMC Health Serv Res. 2017 May 15;17(1):349. doi: 10.1186/s12913-017-2213-4.
Empirical evidence shows that family involvement (FI) can play a pivotal role in the coping and recovery of persons with severe mental illness (SMI). Nevertheless, various studies demonstrate that FI in mental healthcare services is often not (sufficiently) realized. In order to develop more insights, this scoping review gives an overview of how various stakeholders conceptualize, perceive and experience barriers to FI. Central questions are: 1) What are the main barriers to FI reported by the different key stakeholders (i.e. the persons with SMI, their families and the professionals, and 2) What are the differences and similarities between the various stakeholders' perspectives on these barriers.
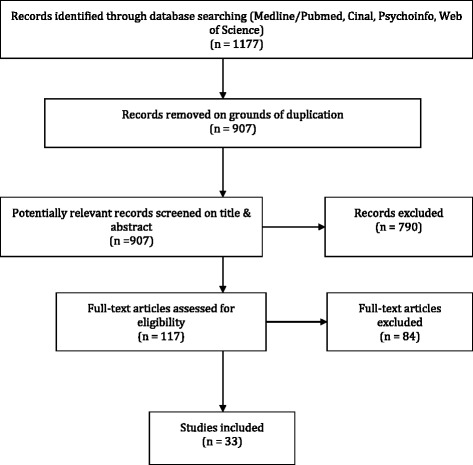
A systematic search into primary studies regarding FI was conducted in four databases: Medline/Pubmed, Cinahl, PsychInfo and Web of Knowledge with the use of a PICO scheme. Thematic analysis focused on stakeholder perspectives (i.e. which stakeholder group reports the barrier) and types of barriers (i.e. which types of barriers are addressed).
Thirty three studies were included. The main barriers reported by the stakeholder groups reveal important similarities and differences between the stakeholder groups and were related to: 1) the person with SMI, 2) the family, 3) the professionals, 4) the organization of care and 5) the culture-paradigm.
Our stakeholder approach elicits the different stakeholders' concepts, presuppositions and experiences of barriers to FI, and gives fundamental insights on how to deal with barriers to FI. The stakeholders differing interpretations and perceptions of the barriers related to FI is closely related to the inherent complexity involved in FI in itself. In order to deal better with these barriers, openly discussing and reflecting upon each other's normative understandings of barriers is needed.
Differences in perceptions of barriers to FI can itself be a barrier. To deal with barriers to FI, a dialogical approach on how the different stakeholders perceive and value FI and its barriers is required. Methods such as moral case deliberation or systematic ethics reflections can be useful.
实证证据表明,家庭参与(FI)在严重精神疾病(SMI)患者的应对和康复中可发挥关键作用。然而,多项研究表明,精神卫生保健服务中的家庭参与往往未(充分)实现。为了深入了解,本范围综述概述了不同利益相关者如何概念化、感知和体验家庭参与的障碍。核心问题是:1)不同关键利益相关者(即SMI患者、其家人和专业人员)报告的家庭参与的主要障碍是什么,以及2)各利益相关者对这些障碍的看法有哪些异同。
使用PICO方案在四个数据库(Medline/Pubmed、Cinahl、PsychInfo和Web of Knowledge)中对有关家庭参与的原始研究进行系统检索。主题分析侧重于利益相关者的观点(即哪个利益相关者群体报告了该障碍)和障碍类型(即涉及哪些类型的障碍)。
纳入了33项研究。利益相关者群体报告的主要障碍揭示了各利益相关者群体之间的重要异同,这些障碍与以下方面有关:1)SMI患者,2)家庭,3)专业人员,4)护理组织,以及5)文化范式。
我们的利益相关者方法引出了不同利益相关者对家庭参与障碍的概念、预设和体验,并就如何应对家庭参与障碍提供了基本见解。利益相关者对与家庭参与相关障碍的不同解释和看法与家庭参与本身固有的复杂性密切相关。为了更好地应对这些障碍,需要公开讨论并反思彼此对障碍的规范性理解。
对家庭参与障碍的认知差异本身可能就是一个障碍。为了应对家庭参与障碍,需要采用一种对话方法,探讨不同利益相关者如何看待和重视家庭参与及其障碍。道德案例审议或系统伦理反思等方法可能会有所帮助。