Rigante M, La Rocca G, Lauretti L, D'Alessandris G Q, Mangiola A, Anile C, Olivi A, Paludetti G
Institute of Otorhinolaryngology, Catholic University School of Medicine, Rome, Italy.
Institute of Neurosurgery, Catholic University School of Medicine, Rome, Italy.
Acta Otorhinolaryngol Ital. 2017 Jun;37(3):237-241. doi: 10.14639/0392-100X-1684.
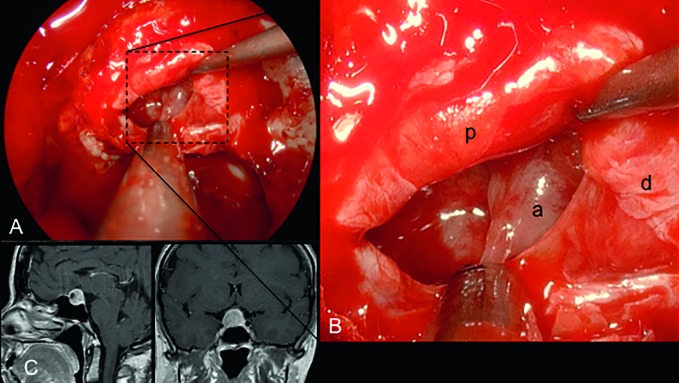
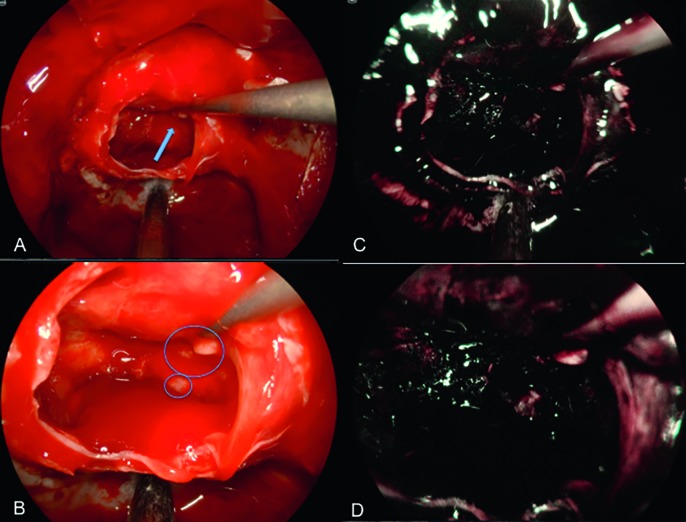
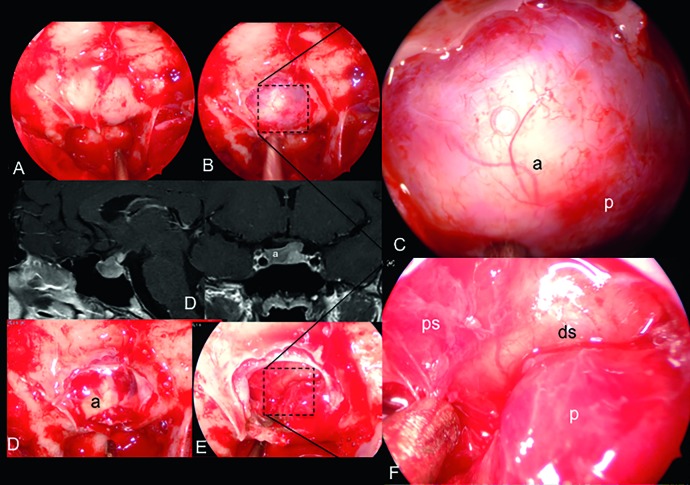
During the last two decades endoscopic skull base surgery observed a continuous technical and technological development 3D endoscopy and ultra High Definition (HD) endoscopy have provided great advances in terms of visualisation and spatial resolution. Ultra-high definition (UHD) 4K systems, recently introduced in the clinical practice, will shape next steps forward especially in skull base surgery field. Patients were operated on through transnasal transsphenoidal endoscopic approaches performed using Olympus NBI 4K UHD endoscope with a 4 mm 0° Ultra Telescope, 300 W xenon lamp (CLV-S400) predisposed for narrow band imaging (NBI) technology connected through a camera head to a high-quality control unit (OTV-S400 - VISERA 4K UHD) (Olympus Corporation, Tokyo, Japan). Two screens are used, one 31" Monitor - (LMD-X310S) and one main ultra-HD 55" screen optimised for UHD image reproduction (LMD-X550S). In selected cases, we used a navigation system (Stealthstation S7, Medtronic, Minneapolis, MN, US). We evaluated 22 pituitary adenomas (86.3% macroadenomas; 13.7% microadenomas). 50% were not functional (NF), 22.8% GH, 18.2% ACTH, 9% PRL-secreting. Three of 22 were recurrences. In 91% of cases we achieved total removal, while in 9% near total resection. A mean follow-up of 187 days and average length of hospitalisation was 3.09 ± 0.61 days. Surgical duration was 128.18± 30.74 minutes. We experienced only 1 case of intraoperative low flow fistula with no further complications. None of the cases required any post- or intraoperative blood transfusion. The visualisation and high resolution of the operative field provided a very detailed view of all anatomical structures and pathologies allowing an improvement in safety and efficacy of the surgical procedure. The operative time was similar to the standard 2D HD and 3D procedures and the physical strain was also comparable to others in terms of ergonomics and weight.
在过去二十年中,内镜颅底手术经历了持续的技术和工艺发展。3D 内镜和超高清(HD)内镜在可视化和空间分辨率方面取得了巨大进展。最近引入临床实践的超高清(UHD)4K 系统将塑造未来的发展方向,特别是在颅底手术领域。患者通过经鼻经蝶内镜入路进行手术,使用 Olympus NBI 4K UHD 内镜,配备 4 毫米 0°超望远镜、300 瓦氙灯(CLV-S400),该氙灯专为窄带成像(NBI)技术设计,通过摄像头连接到高质量控制单元(OTV-S400 - VISERA 4K UHD)(日本东京奥林巴斯公司)。使用两个屏幕,一个 31 英寸显示器(LMD-X310S)和一个专为 UHD 图像再现优化的主超高清 55 英寸屏幕(LMD-X550S)。在选定的病例中,我们使用了导航系统(美国明尼阿波利斯美敦力公司的 Stealthstation S7)。我们评估了 22 例垂体腺瘤(86.3%为大腺瘤;13.7%为微腺瘤)。50%为无功能型(NF),22.8%为生长激素(GH)型,18.2%为促肾上腺皮质激素(ACTH)型,9%为泌乳素(PRL)分泌型。22 例中有 3 例为复发病例。91%的病例实现了全切,9%为近全切。平均随访 187 天,平均住院时间为 3.09±0.61 天。手术时长为 128.18±30.74 分钟。我们仅遇到 1 例术中低流量瘘,无进一步并发症。所有病例均未在术中或术后输血。手术视野的可视化和高分辨率提供了所有解剖结构和病变的非常详细的视图,提高了手术的安全性和有效性。手术时间与标准的 2D HD 和 3D 手术相似,在人体工程学和重量方面的体力消耗也与其他手术相当。