Aggarwal Rakesh, Chen Qiushi, Goel Amit, Seguy Nicole, Pendse Razia, Ayer Turgay, Chhatwal Jagpreet
Department of Gastroenterology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India.
Massachusetts General Hospital Institute for Technology Assessment, Boston, Massachusetts, United States of America.
PLoS One. 2017 May 17;12(5):e0176503. doi: 10.1371/journal.pone.0176503. eCollection 2017.
BACKGROUND & AIMS: Availability of directly-acting antivirals (DAAs) has changed the treatment landscape of hepatitis C virus (HCV) infection. The high price of DAAs has restricted their use in several countries. However, in some countries such as India, generic DAAs are available at much cheaper price. This study examined whether generic DAAs could be cost-saving and how long it would take for the treatment to become cost-saving/effective.
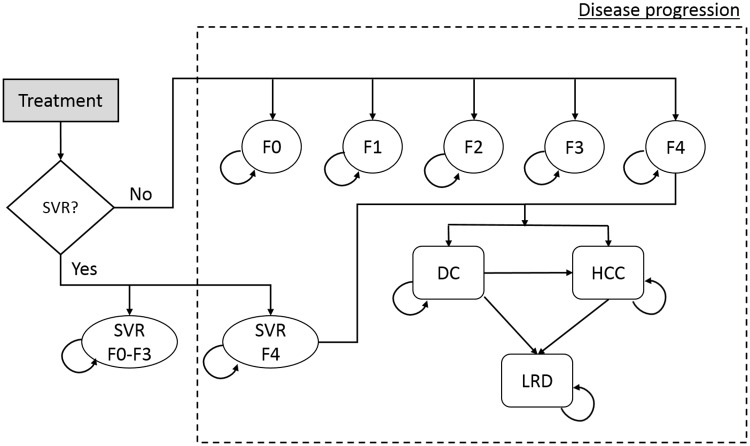
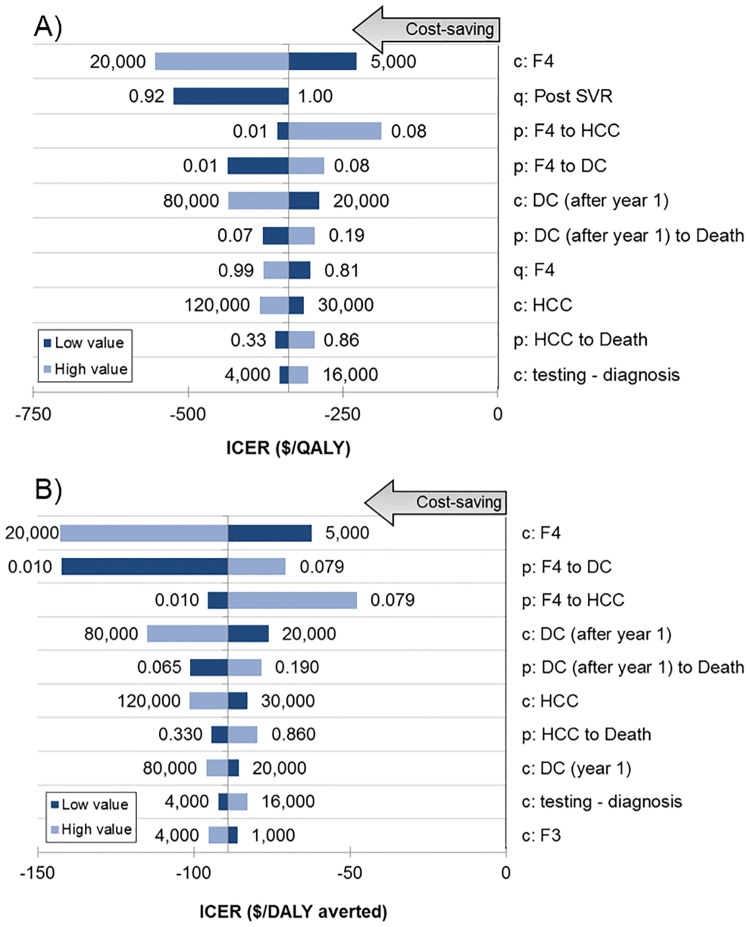
A previously-validated, mathematical model was adapted to the HCV-infected population in India to compare the outcomes of no treatment versus treatment with DAAs. Model parameters were estimated from published studies. Cost-effectiveness of HCV treatment using available DAAs was calculated, using a payer's perspective. We estimated quality-adjusted life years (QALYs), disability-adjusted life years (DALYs), total costs, and incremental cost-effectiveness ratio of DAAs versus no treatment. One-way and probabilistic sensitivity analyses were conducted.
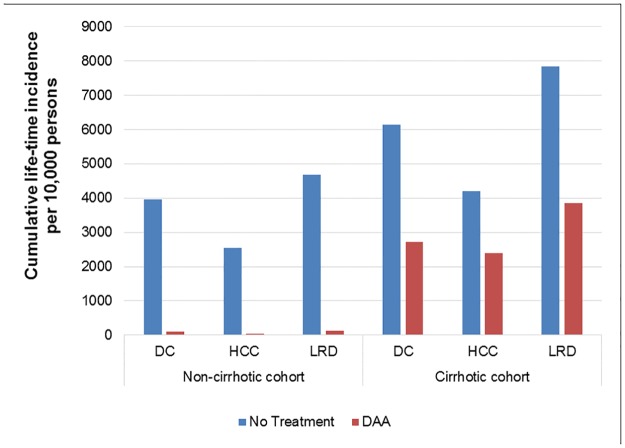
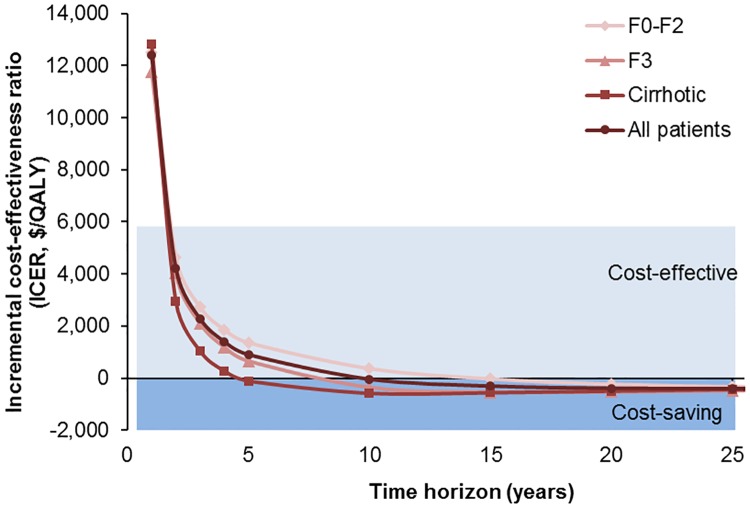
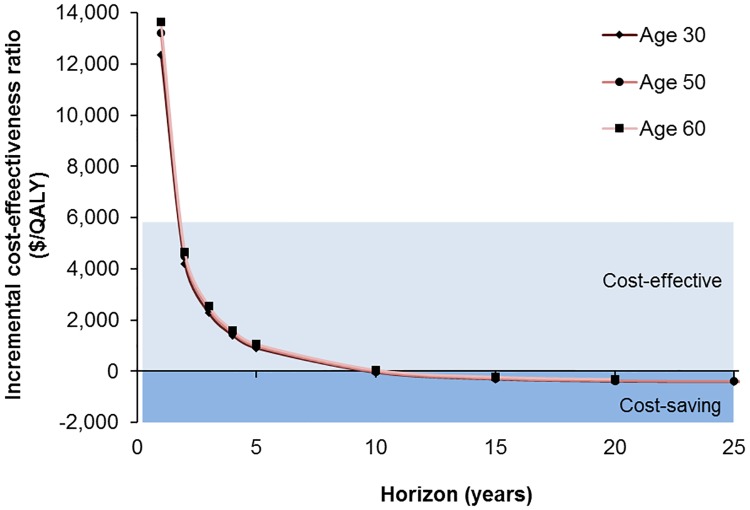
Compared with no treatment, the use of generic DAAs in Indian HCV patients would increase the life expectancy by 8.02 years, increase QALYs by 3.89, avert 19.07 DALYs, and reduce the lifetime healthcare costs by $1,309 per-person treated. Treatment became cost-effective within 2 years, and cost-saving within 10 years of its initiation overall and within 5 years in persons with cirrhosis. Treating 10,000 HCV-infected persons could prevent 3400-3850 decompensated cirrhosis, 1800-2500 HCC, and 4000-4550 liver-related deaths. The results were sensitive to the costs of DAAs, pre- and post-treatment diagnostic tests and management of cirrhosis, and quality of life after sustained virologic response.
Treatment with generic DAAs available in India will improve patient outcomes, provide a good value for money within 2 years, and be ultimately cost-saving. Therefore, in this and similar settings, HCV treatment should be a priority from a public health as well an economic perspective.
直接抗病毒药物(DAAs)的出现改变了丙型肝炎病毒(HCV)感染的治疗格局。DAAs的高昂价格限制了其在多个国家的使用。然而,在印度等一些国家,可以以低得多的价格获得仿制药。本研究探讨了仿制药是否能节省成本,以及治疗需要多长时间才能实现成本节省/有效。
将一个先前验证过的数学模型应用于印度的HCV感染人群,以比较不治疗与使用DAAs治疗的结果。模型参数根据已发表的研究进行估计。从支付方的角度计算使用现有DAAs进行HCV治疗的成本效益。我们估计了质量调整生命年(QALYs)、伤残调整生命年(DALYs)、总成本以及DAAs与不治疗相比的增量成本效益比。进行了单因素和概率敏感性分析。
与不治疗相比,在印度HCV患者中使用仿制药将使预期寿命延长8.02年,QALYs增加3.89,避免19.07个DALYs,并使每位接受治疗的患者终身医疗费用降低1309美元。治疗在2年内变得具有成本效益,总体上在开始治疗后的10年内实现成本节省,而在肝硬化患者中则在治疗5年内实现成本节省。治疗10000名HCV感染者可预防3400 - 3850例失代偿性肝硬化、1800 - 2500例肝癌以及4000 - 4550例肝脏相关死亡。结果对DAAs的成本、治疗前后的诊断测试以及肝硬化的管理以及持续病毒学应答后的生活质量敏感。
在印度可获得的仿制药进行治疗将改善患者预后,在2年内提供良好的性价比,并最终节省成本。因此,在这种及类似情况下,从公共卫生和经济角度来看,HCV治疗都应成为优先事项。