Cho Soo Young, Park Jun Won, Liu Yang, Park Young Soo, Kim Ju Hee, Yang Hanna, Um Hyejin, Ko Woo Ri, Lee Byung Il, Kwon Sun Young, Ryu Seung Wan, Kwon Chae Hwa, Park Do Youn, Lee Jae-Hyuk, Lee Sang Il, Song Kyu Sang, Hur Hoon, Han Sang-Uk, Chang Heekyung, Kim Su-Jin, Kim Byung-Sik, Yook Jeong-Hwan, Yoo Moon-Won, Kim Beom-Su, Lee In-Seob, Kook Myeong-Cherl, Thiessen Nina, He An, Stewart Chip, Dunford Andrew, Kim Jaegil, Shih Juliann, Saksena Gordon, Cherniack Andrew D, Schumacher Steven, Weiner Amaro-Taylor, Rosenberg Mara, Getz Gad, Yang Eun Gyeong, Ryu Min-Hee, Bass Adam J, Kim Hark Kyun
National Cancer Center, Goyang, Gyeonggi, Republic of Korea.
Cancer Program, The Broad Institute of MIT and Harvard, Cambridge, Massachusetts.
Gastroenterology. 2017 Aug;153(2):536-549.e26. doi: 10.1053/j.gastro.2017.05.012. Epub 2017 May 15.
BACKGROUND & AIMS: Early-onset gastric cancer, which develops in patients younger than most gastric cancers, is usually detected at advanced stages, has diffuse histologic features, and occurs more frequently in women. We investigated somatic genomic alterations associated with the unique characteristics of sporadic diffuse gastric cancers (DGCs) from younger patients.
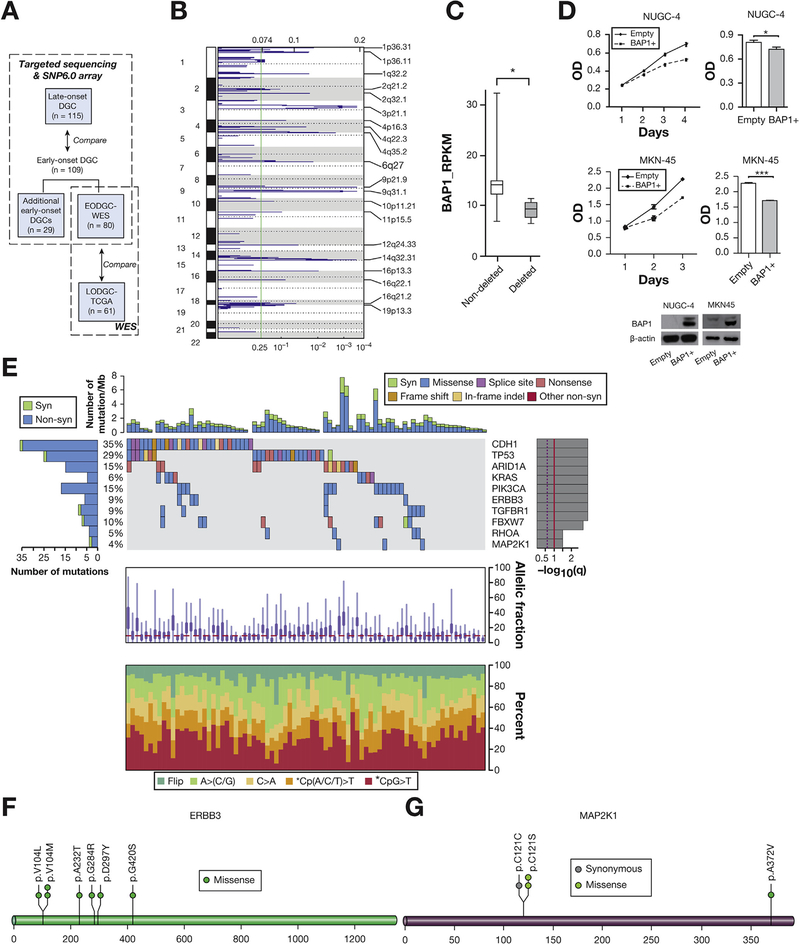
We conducted whole exome and RNA sequence analyses of 80 resected DGC samples from patients 45 years old or younger in Korea. Patients with pathogenic germline mutations in CDH1, TP53, and ATM were excluded from the onset of this analysis, given our focus on somatic alterations. We used MutSig2CV to evaluate the significance of mutated genes. We recruited 29 additional early-onset Korean DGC samples and performed SNP6.0 array and targeted sequencing analyses of these 109 early-onset DGC samples (54.1% female, median age, 38 years). We compared the SNP6.0 array and targeted sequencing data of the 109 early-onset DGC samples with those from diffuse-type stomach tumor samples collected from 115 patients in Korea who were 46 years or older (late onset) at the time of diagnosis (controls; 29.6% female, median age, 67 years). We compared patient survival times among tumors from different subgroups and with different somatic mutations. We performed gene silencing of RHOA or CDH1 in DGC cells with small interfering RNAs for cell-based assays.
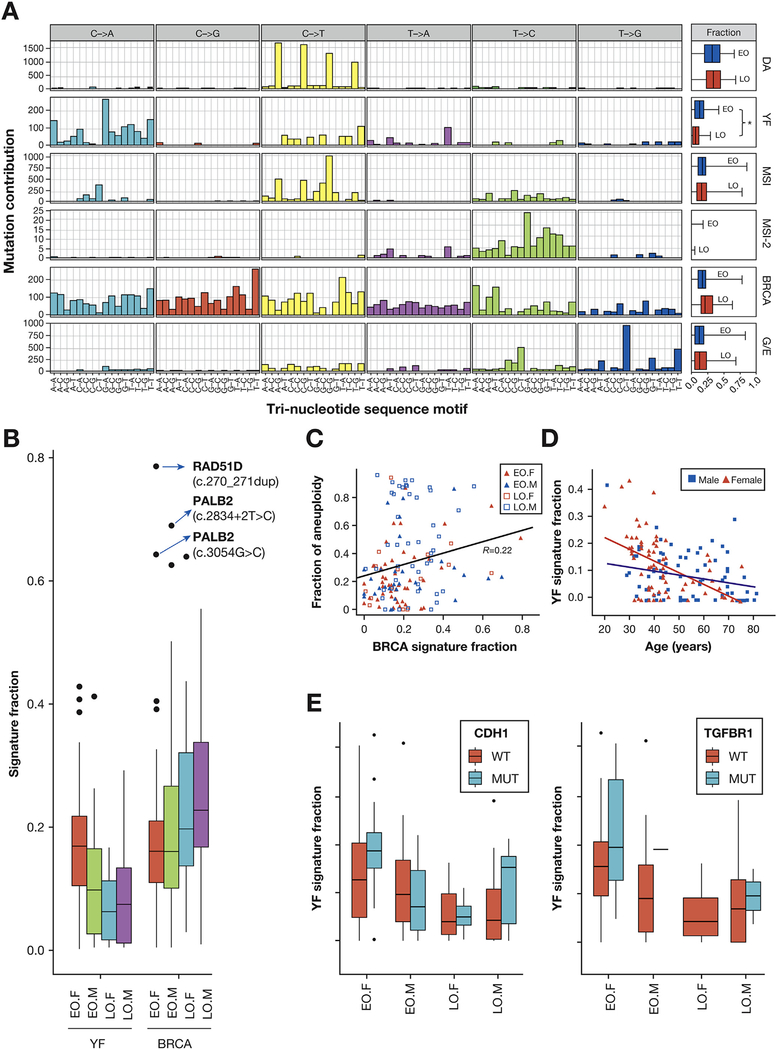
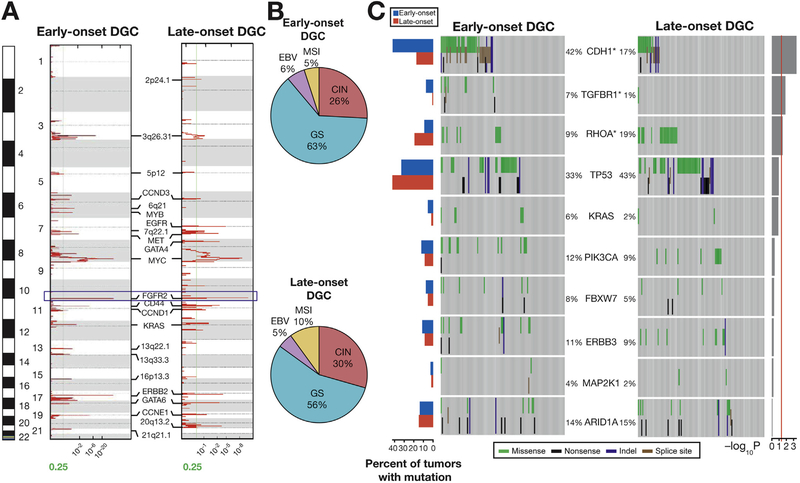
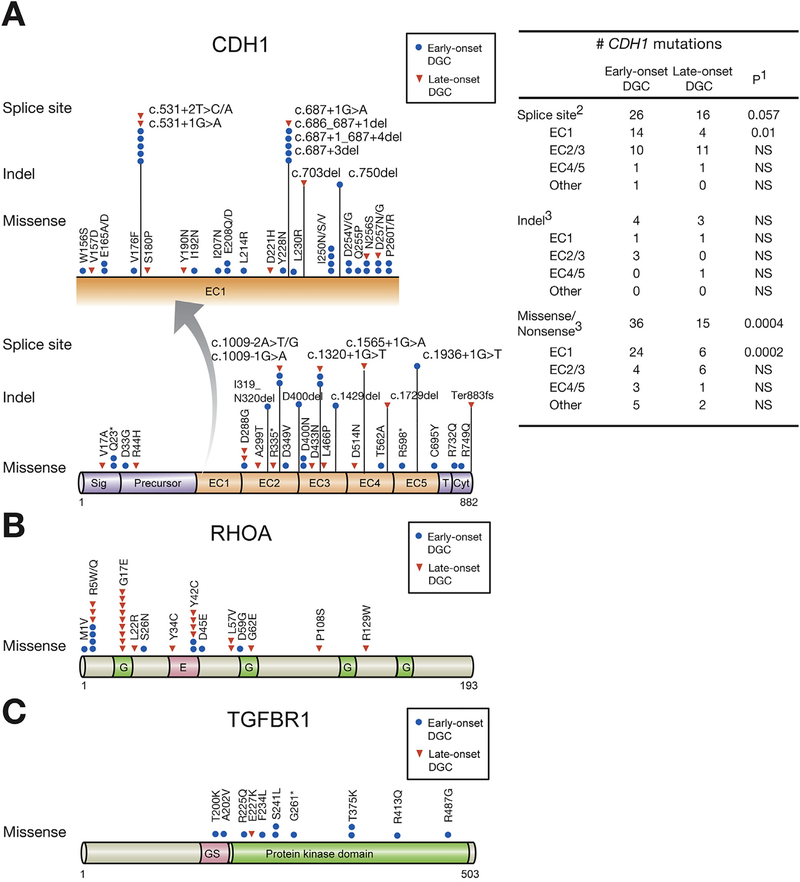
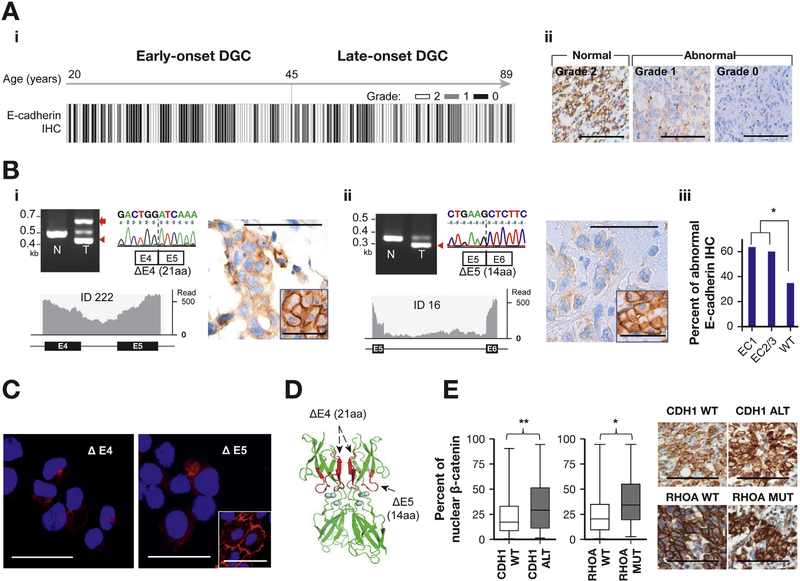
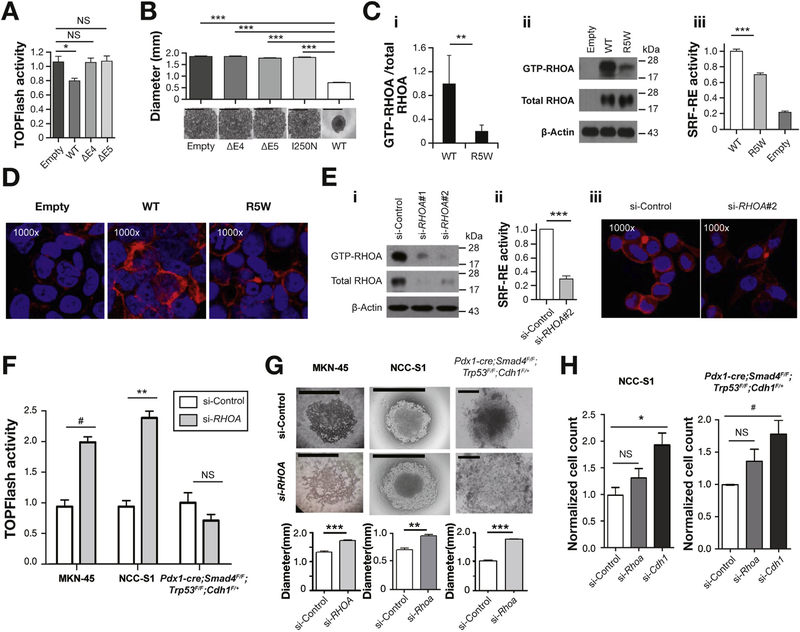
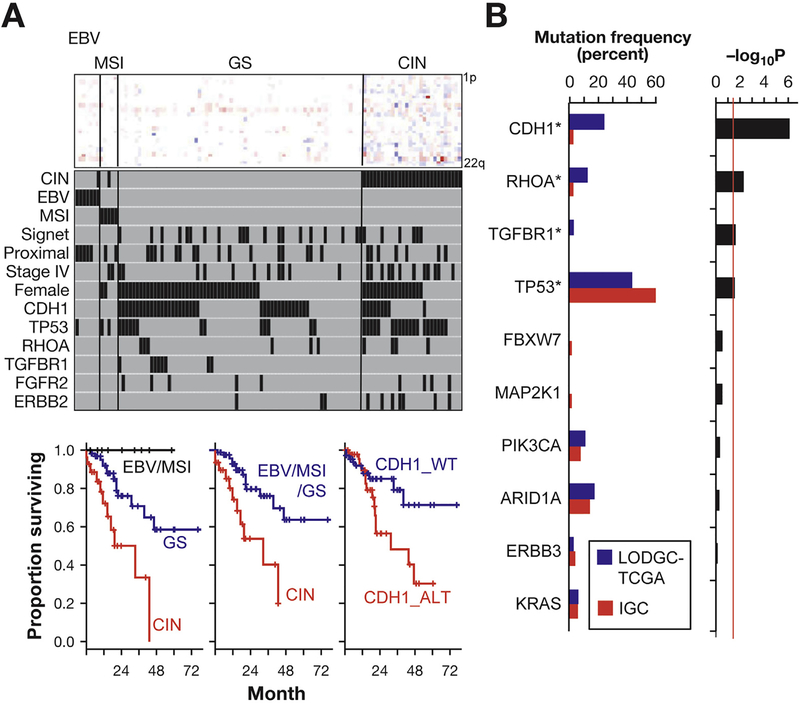
We identified somatic mutations in the following genes in a significant number of early-onset DGCs: the cadherin 1 gene (CDH1), TP53, ARID1A, KRAS, PIK3CA, ERBB3, TGFBR1, FBXW7, RHOA, and MAP2K1. None of 109 early-onset DGC cases had pathogenic germline CDH1 mutations. A higher proportion of early-onset DGCs had mutations in CDH1 (42.2%) or TGFBR1 (7.3%) compared with control DGCs (17.4% and 0.9%, respectively) (P < .001 and P = .014 for CDH1 and TGFBR1, respectively). In contrast, a smaller proportion of early-onset DGCs contained mutations in RHOA (9.2%) than control DGCs (19.1%) (P = .033). Late-onset DGCs in The Cancer Genome Atlas also contained less frequent mutations in CDH1 and TGFBR1 and more frequent RHOA mutations, compared with early-onset DGCs. Early-onset DGCs from women contained significantly more mutations in CDH1 or TGFBR1 than early-onset DGCs from men. CDH1 alterations, but not RHOA mutations, were associated with shorter survival times in patients with early-onset DGCs (hazard ratio, 3.4; 95% confidence interval, 1.5-7.7). RHOA activity was reduced by an R5W substitution-the RHOA mutation most frequently detected in early-onset DGCs. Silencing of CDH1, but not RHOA, increased migratory activity of DGC cells.
In an integrative genomic analysis, we found higher proportions of early-onset DGCs to contain somatic mutations in CDH1 or TGFBR1 compared with late-onset DGCs. However, a smaller proportion of early-onset DGCs contained somatic mutations in RHOA than late-onset DGCs. CDH1 alterations, but not RHOA mutations, were associated with shorter survival times of patients, which might account for the aggressive clinical course of early-onset gastric cancer. Female predominance in early-onset gastric cancer may be related to relatively high rates of somatic CDH1 and TGFBR1 mutations in this population.
早发性胃癌在比大多数胃癌患者更年轻的人群中发病,通常在晚期被发现,具有弥漫性组织学特征,且在女性中更为常见。我们研究了与年轻患者散发性弥漫性胃癌(DGC)独特特征相关的体细胞基因组改变。
我们对韩国45岁及以下患者的80例切除的DGC样本进行了全外显子组和RNA序列分析。鉴于我们关注的是体细胞改变,因此在分析开始时就排除了携带CDH1、TP53和ATM致病种系突变的患者。我们使用MutSig2CV评估突变基因的显著性。我们又招募了29例韩国早发性DGC样本,并对这109例早发性DGC样本(54.1%为女性,中位年龄38岁)进行了SNP6.0芯片和靶向测序分析。我们将这109例早发性DGC样本的SNP6.0芯片和靶向测序数据与从韩国115例诊断时年龄在46岁及以上(晚发性)的弥漫型胃肿瘤样本(对照组;29.6%为女性,中位年龄67岁)的数据进行了比较。我们比较了不同亚组肿瘤以及具有不同体细胞突变的肿瘤患者的生存时间。我们使用小干扰RNA对DGC细胞中的RHOA或CDH1进行基因沉默,以进行基于细胞的检测。
我们在大量早发性DGC中鉴定出以下基因的体细胞突变:钙黏蛋白1基因(CDH1)、TP53、ARID1A、KRAS、PIK3CA、ERBB3、TGFBR1、FBXW7、RHOA和MAP2K1。109例早发性DGC病例均无致病种系CDH1突变。与对照DGC相比,早发性DGC中CDH1(42.2%)或TGFBR1(7.3%)发生突变的比例更高(CDH1和TGFBR1分别为P <.001和P = 0.014)。相比之下,早发性DGC中RHOA发生突变的比例(9.2%)低于对照DGC(19.1%)(P = 0.033)。与早发性DGC相比,癌症基因组图谱中的晚发性DGC中CDH1和TGFBR1的突变频率也较低,而RHOA的突变频率较高。早发性DGC女性患者中CDH1或TGFBR1的突变明显多于早发性DGC男性患者。在早发性DGC患者中,CDH1改变而非RHOA突变与较短的生存时间相关(风险比,3.4;95%置信区间,1.5 - 7.7)。RHOA活性因R5W替代而降低——这是早发性DGC中最常检测到的RHOA突变。沉默CDH1而非RHOA可增加DGC细胞的迁移活性。
在一项综合基因组分析中,我们发现与晚发性DGC相比,早发性DGC中CDH1或TGFBR1体细胞突变的比例更高。然而,早发性DGC中RHOA体细胞突变的比例低于晚发性DGC。CDH1改变而非RHOA突变与患者较短的生存时间相关,这可能解释了早发性胃癌的侵袭性临床病程。早发性胃癌中女性占优势可能与该人群中CDH1和TGFBR1体细胞突变率相对较高有关。