Blankenstein Oliver, Snajderova Marta, Blair Jo, Pournara Effie, Pedersen Birgitte Tønnes, Petit Isabelle Oliver
Center for Chronic Sick Children, Institute for Experimental Paediatric Endocrinology, Charité - Universitätsmedizin Berlin, Berlin, Germany.
2nd Faculty of Medicine, Charles University and University Hospital Motol, Prague, Czech Republic.
Eur J Endocrinol. 2017 Aug;177(2):145-155. doi: 10.1530/EJE-16-1055. Epub 2017 May 18.
To describe real-life dosing patterns in children with growth hormone deficiency (GHD), born small for gestational age (SGA) or with Turner syndrome (TS) receiving growth hormone (GH) and enrolled in the NordiNet International Outcome Study (IOS; Nbib960128) between 2006 and 2016.
This non-interventional, multicentre study included paediatric patients diagnosed with GHD (isolated (IGHD) or multiple pituitary hormone deficiency (MPHD)), born SGA or with TS and treated according to everyday clinical practice from the Czech Republic (IGHD/MPHD/SGA/TS: = 425/61/316/119), France ( = 1404/188/970/206), Germany ( = 2603/351/1387/411) and the UK ( = 259/60/87/35).
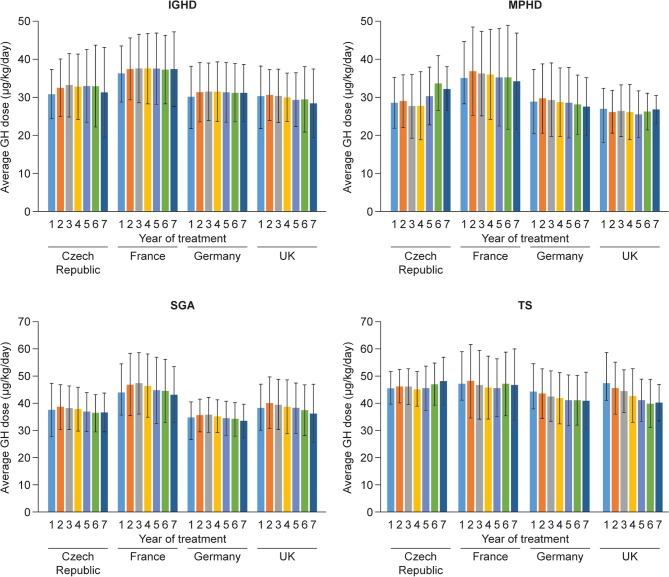
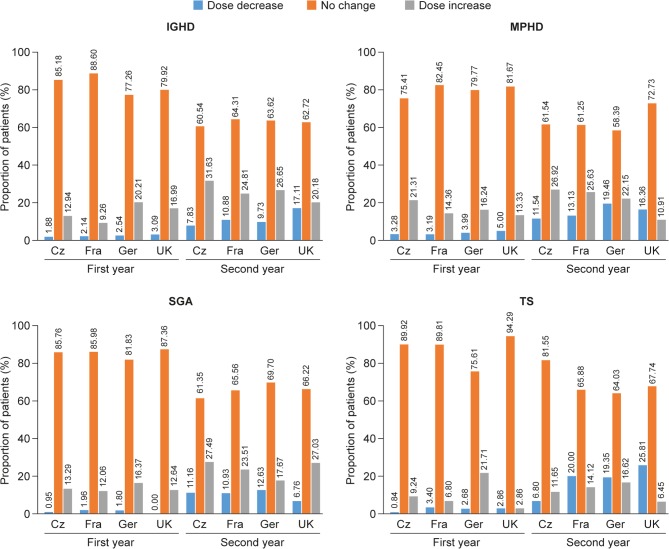
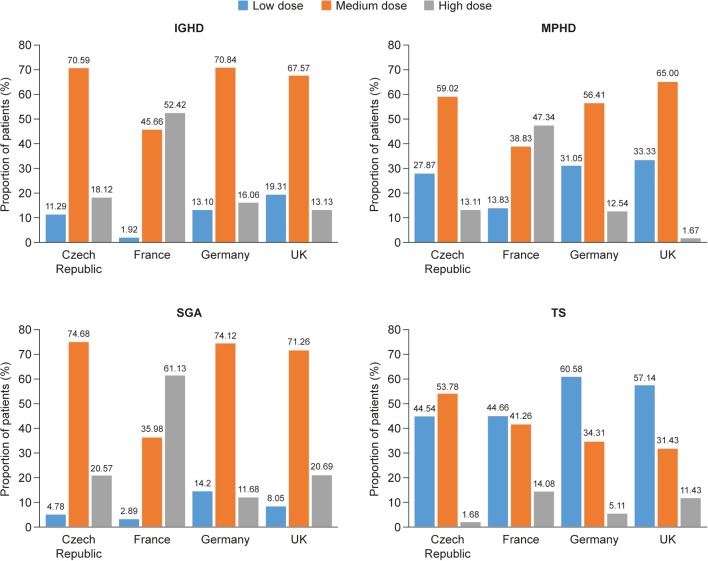
GH dosing was compared descriptively across countries and indications. Proportions of patients by GH dose group (low/medium/high) or GH dose change (decrease/increase/no change) during years 1 and 2 were also evaluated across countries and indications.
In the Czech Republic, GH dosing was generally within recommended levels. In France, average GH doses were higher for patients with IGHD, MPHD and SGA than in other countries. GH doses in TS tended to be at the lower end of the recommended label range, especially in Germany and the UK; the majority of patients were in the low-dose group. A significant inverse association between baseline height standard deviation score and GH dose was shown ( < 0.05); shorter patients received higher doses. Changes in GH dose, particularly increases, were more common in the second (40%) than in the first year (25%).
GH dosing varies considerably across countries and indications. In particular, almost half of girls with TS received GH doses below practice guidelines and label recommendations.
描述2006年至2016年间参与NordiNet国际结局研究(IOS;Nbib960128)、患有生长激素缺乏症(GHD)、出生时小于胎龄(SGA)或患有特纳综合征(TS)并接受生长激素(GH)治疗的儿童的实际用药模式。
这项非干预性多中心研究纳入了被诊断为GHD(孤立性生长激素缺乏症(IGHD)或多种垂体激素缺乏症(MPHD))、出生时小于胎龄或患有TS并按照捷克共和国(IGHD/MPHD/SGA/TS:=425/61/316/119)、法国(=1404/188/970/206)、德国(=2603/351/1387/411)和英国(=259/60/87/35)的日常临床实践进行治疗的儿科患者。
对各国和各适应症的生长激素给药情况进行描述性比较。还评估了第1年和第2年期间按生长激素剂量组(低/中/高)或生长激素剂量变化(减少/增加/无变化)划分的患者比例,涉及各国和各适应症。
在捷克共和国,生长激素给药一般在推荐水平内。在法国,IGHD、MPHD和SGA患者的平均生长激素剂量高于其他国家。TS患者的生长激素剂量往往处于推荐标签范围的下限,尤其是在德国和英国;大多数患者属于低剂量组。基线身高标准差评分与生长激素剂量之间存在显著的负相关(<0.05);身材较矮的患者接受的剂量较高。生长激素剂量的变化,尤其是增加,在第2年(40%)比第1年(25%)更为常见。
生长激素给药在各国和各适应症之间存在很大差异。特别是,几乎一半的TS女孩接受的生长激素剂量低于实践指南和标签建议。