Gray Ronan T, Loughrey Maurice B, Bankhead Peter, Cardwell Chris R, McQuaid Stephen, O'Neill Roisin F, Arthur Kenneth, Bingham Victoria, McGready Claire, Gavin Anna T, James Jacqueline A, Hamilton Peter W, Salto-Tellez Manuel, Murray Liam J, Coleman Helen G
Cancer Epidemiology and Health Services Research Group, Centre for Public Health, Queen's University Belfast, Belfast, Northern Ireland, UK.
Northern Ireland Molecular Pathology Laboratory, Centre for Cancer Research and Cell Biology, Queen's University Belfast, Belfast, Northern Ireland, UK.
Br J Cancer. 2017 Jun 6;116(12):1652-1659. doi: 10.1038/bjc.2017.139. Epub 2017 May 18.
Statin use after colorectal cancer diagnosis may improve survival but evidence from observational studies is conflicting. The anti-cancer effect of statins may be restricted to certain molecular subgroups. In this population-based cohort study, the interaction between p53 and 3-hydroxy-3-methylglutaryl coenzyme-A reductase (HMGCR) expression, KRAS mutations, and the association between statin use and colon cancer survival was assessed.
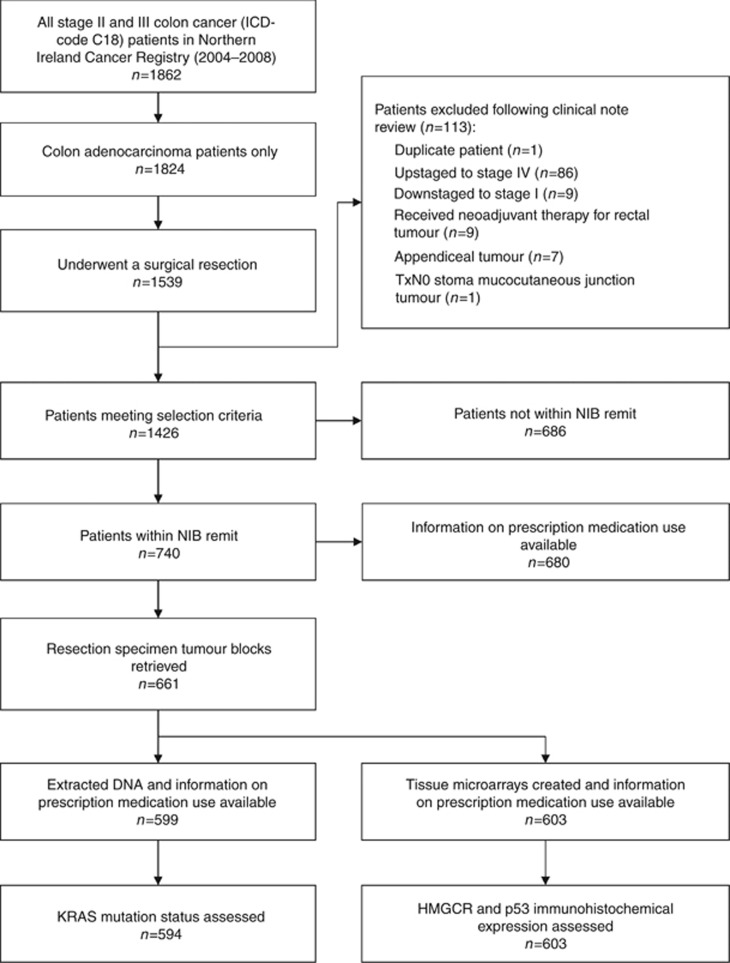
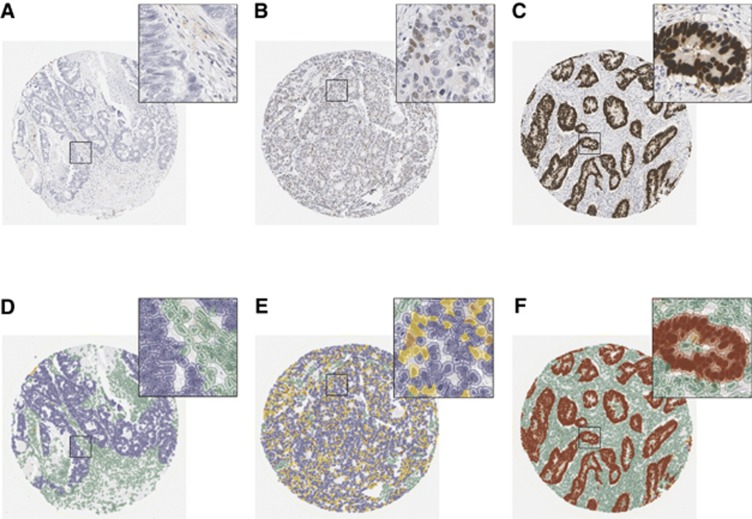
The cohort consisted of 740 stage II and III colon cancer patients diagnosed between 2004 and 2008. Statin use was determined through clinical note review. Tissue blocks were retrieved to determine immunohistochemical expression of p53 and HMGCR in tissue microarrays and the presence of KRAS mutations in extracted DNA. Cox proportional hazards models were used to calculate hazard ratios (HRs) and 95% confidence intervals (CIs) for colorectal cancer-specific and overall survival.
Statin use was not associated with improved cancer-specific survival in this cohort (HR=0.91, 95% CI 0.64-1.28). Statin use was also not associated with improved survival when the analyses were stratified by tumour p53 (wild-type HR=1.31, 95% CI 0.67-2.56 vs aberrant HR=0.80, 95% CI 0.52-1.24), HMGCR (HMGCR-high HR=0.69, 95% CI 0.40-1.18 vs HMGCR-low HR=1.10, 95% CI 0.66-1.84), and KRAS (wild-type HR=0.73, 95% CI 0.44-1.19 vs mutant HR=1.21, 95% CI 0.70-2.21) status.
Statin use was not associated with improved survival either independently or when stratified by potential mevalonate pathway biomarkers in this population-based cohort of colon cancer patients.
结直肠癌诊断后使用他汀类药物可能会提高生存率,但观察性研究的证据相互矛盾。他汀类药物的抗癌作用可能仅限于某些分子亚组。在这项基于人群的队列研究中,评估了p53与3-羟基-3-甲基戊二酰辅酶A还原酶(HMGCR)表达、KRAS突变之间的相互作用,以及他汀类药物使用与结肠癌生存率之间的关联。
该队列由2004年至2008年间诊断出的740例II期和III期结肠癌患者组成。通过临床记录回顾确定他汀类药物的使用情况。检索组织块以确定组织微阵列中p53和HMGCR的免疫组化表达以及提取DNA中KRAS突变的存在情况。使用Cox比例风险模型计算结直肠癌特异性生存率和总生存率的风险比(HR)和95%置信区间(CI)。
在该队列中,使用他汀类药物与改善癌症特异性生存率无关(HR=0.91,95%CI 0.64-1.28)。当按肿瘤p53(野生型HR=1.31,95%CI 0.67-2.56对比异常HR=0.80,95%CI 0.52-1.24)、HMGCR(HMGCR高表达HR=0.69,95%CI 0.40-1.18对比HMGCR低表达HR=1.10,95%CI 0.66-1.84)和KRAS(野生型HR=0.73,95%CI 0.44-1.19对比突变型HR=1.21,95%CI 0.70-2.21)状态进行分层分析时,使用他汀类药物也与生存率改善无关。
在这个基于人群的结肠癌患者队列中,使用他汀类药物无论是独立使用还是按潜在甲羟戊酸途径生物标志物分层使用,均与生存率改善无关。