Jiao Wei-Ping, Zhang Lei
Department of Ultrasound, Beijing Xuanwu Hospital, Capital Medical University, Beijing 100053, China.
Department of Cardiology, Beijing Xuanwu Hospital, Capital Medical University, Beijing 100053, China.
Chin Med J (Engl). 2017 Jun 5;130(11):1309-1313. doi: 10.4103/0366-6999.206339.
Previous studies have demonstrated that ultrasonography is the recommended imaging modality for preoperative staging of papillary thyroid carcinomas (PTCs). However, only a few studies have kept watch on preoperative evaluation of capsular invasion (CI) or extracapsular extension (ECE) and cervical lymph node metastasis using preoperative ultrasonography. This study aimed to investigate the relationship between the CI or ECE and the cervical lymph node metastasis in PTCs using preoperative ultrasonography and postoperative pathology in Chinese patients.
The data of preoperative ultrasonography and postoperative pathology of 166 patients who had a definitive diagnosis of PTCs from October 2011 to July 2014 at Xuanwu Hospital, Beijing were collected and reviewed. Preoperative ultrasonic parameters of thyroid nodules were compared with those of postoperative pathological diagnoses. All the patients were divided into bilateral PTCs group (n = 42, 78 nodules) and unilateral PTCs group (n = 124, 124 nodules), and the data of the nodule sizes, CI or ECE, and cervical lymph node metastasis by preoperative ultrasonography were compared between two groups.
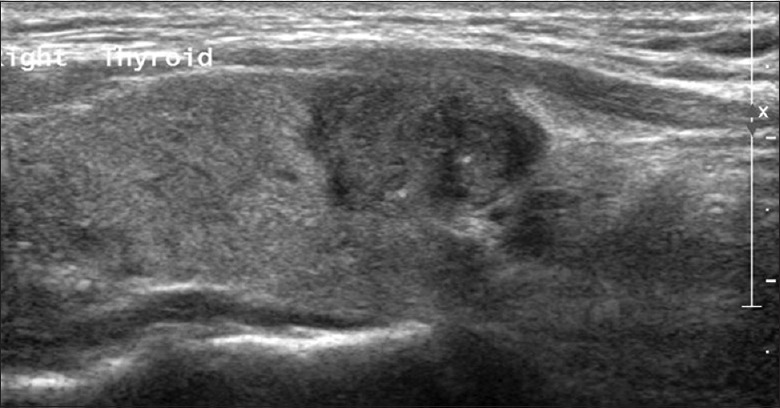
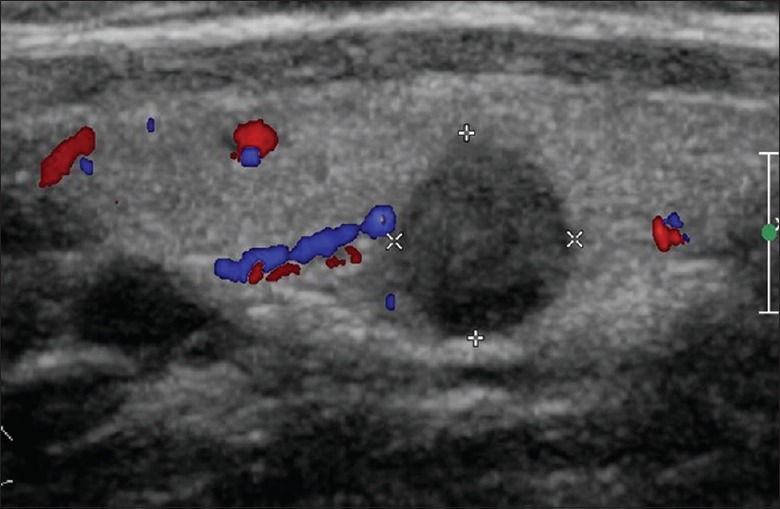
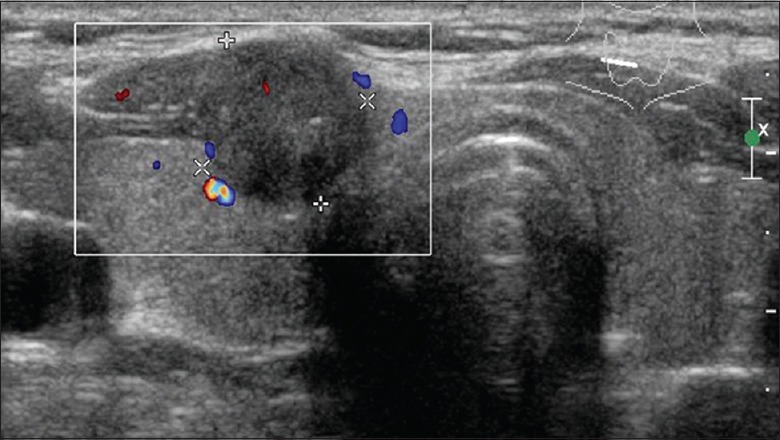
A total of 202 nodules of 166 patients which were confirmed by preoperative ultrasonography and postoperative pathology were analyzed. Hypoechogenicity (n = 201, 99.5%) and irregular margins (n = 167, 82.7%) were the main ultrasonic characteristics of PTCs. A significant moderate agreement between preoperative ultrasonic examination and postoperative pathology for CI or ECE (κ = 0.622, P< 0.001) was observed. The diagnostic sensitivity was 92.0%, and specificity was 71.1%. In bilateral PTCs group, 81.0% had CI or ECE, and 61.9% had cervical lymph node metastasis. In unilateral PTCs group, 76.6% had CI or ECE, and 58.1% had cervical lymph node metastasis. There were no significant differences in the incidence of CI or ECE and cervical lymph node metastasis between two groups (all P > 0.05).
Ultrasonography was proved to be a valuable method for preoperative diagnosis of PTCs. Hypoechogenicity and irregular margins were strongly associated with PTCs. CI or ECE in unilateral PTCs strongly implied the cervical lymph node metastasis. Therefore, the cervical lymph nodes should be carefully examined by ultrasonography in patients with PTCs.
既往研究表明,超声检查是推荐用于甲状腺乳头状癌(PTC)术前分期的影像学检查方法。然而,仅有少数研究关注术前超声检查对甲状腺被膜侵犯(CI)或包膜外扩展(ECE)及颈部淋巴结转移的评估。本研究旨在通过术前超声检查及术后病理,探讨中国PTC患者中CI或ECE与颈部淋巴结转移之间的关系。
收集并回顾2011年10月至2014年7月在北京宣武医院确诊为PTC的166例患者的术前超声检查及术后病理数据。将甲状腺结节的术前超声参数与术后病理诊断结果进行比较。所有患者分为双侧PTC组(n = 42,78个结节)和单侧PTC组(n = 124,124个结节),比较两组术前超声检查的结节大小、CI或ECE及颈部淋巴结转移情况。
对166例患者经术前超声检查及术后病理证实的202个结节进行分析。低回声(n = 201,99.5%)和边界不规则(n = 167,82.7%)是PTC的主要超声特征。术前超声检查与术后病理对CI或ECE的诊断有显著的中度一致性(κ = 0.622,P < 0.001)。诊断敏感性为92.0%,特异性为71.1%。双侧PTC组中,81.0%有CI或ECE,61.9%有颈部淋巴结转移。单侧PTC组中,76.6%有CI或ECE,58.1%有颈部淋巴结转移。两组间CI或ECE及颈部淋巴结转移的发生率无显著差异(均P > 0.05)。
超声检查被证明是PTC术前诊断的一种有价值的方法。低回声和边界不规则与PTC密切相关。单侧PTC中的CI或ECE强烈提示颈部淋巴结转移。因此,PTC患者应通过超声仔细检查颈部淋巴结。