Hu Jiachang, Wang Yimei, Geng Xuemei, Chen Rongyi, Zhang Pan, Lin Jing, Teng Jie, Zhang Xiaoyan, Ding Xiaoqiang
Division of Nephrology, Zhongshan Hospital, Shanghai Medical College, Fudan University, Shanghai, China (mainland).
Shanghai Institute of Kidney and Dialysis, Shanghai, China (mainland).
Med Sci Monit. 2017 May 21;23:2408-2425. doi: 10.12659/msm.902032.
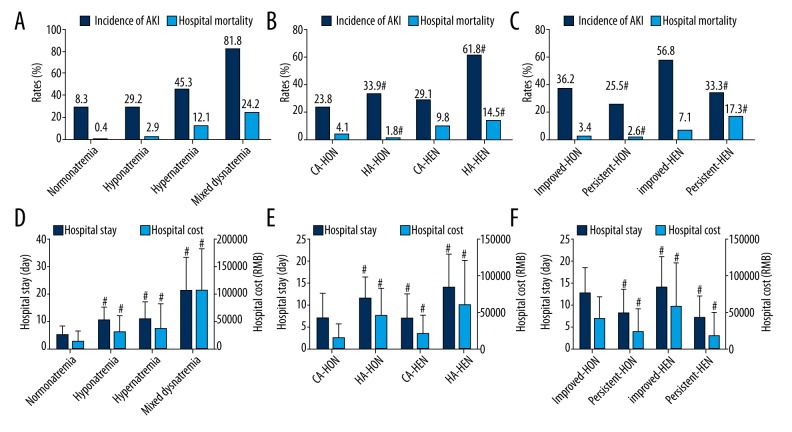
BACKGROUND Dysnatremia is a risk factor for poor outcomes. We aimed to describe the prevalence and outcomes of various dysnatremia in hospitalized patients. High-risk patients must be identified to improve the prognosis of dysnatremia. MATERIAL AND METHODS This prospective study included all adult patients admitted consecutively to a university hospital between October 1, 2014 and September 30, 2015. RESULTS All 90 889 patients were included in this study. According to the serum sodium levels during hospitalization, the incidence of hyponatremia and hypernatremia was 16.8% and 1.9%, respectively. Mixed dysnatremia, which was defined when both hyponatremia and hypernatremia happened in the same patient during hospitalization, took place in 0.3% of patients. The incidence of dysnatremia was different in various underlying diseases. Multiple logistic regression analyses showed that all kinds of dysnatremia were independently associated with hospital mortality. The following dysnatremias were strong predictors of hospital mortality: mixed dysnatremia (OR 22.344, 95% CI 15.709-31.783, P=0.000), hypernatremia (OR 13.387, 95% CI 10.642-16.840, P=0.000), and especially hospital-acquired (OR 16.216, 95% CI 12.588-20.888, P=0.000) and persistent (OR 22.983, 95% CI 17.554-30.092, P=0.000) hypernatremia. Hyponatremia was also a risk factor for hospital mortality (OR 2.225, 95% CI 1.857-2.667). However, the OR increased to 56.884 (95% CI 35.098-92.193) if hyponatremia was over-corrected to hypernatremia. CONCLUSIONS Dysnatremia was independently associated with poor outcomes. Hospital-acquired and persistent hypernatremia were strong risk factors for hospital mortality. Effective prevention and proper correction of dysnatremia in high-risk patients may reduce the hospital mortality.
钠代谢紊乱是不良预后的一个危险因素。我们旨在描述住院患者各种钠代谢紊乱的患病率及预后情况。必须识别出高危患者以改善钠代谢紊乱的预后。
这项前瞻性研究纳入了2014年10月1日至2015年9月30日期间连续入住一所大学医院的所有成年患者。
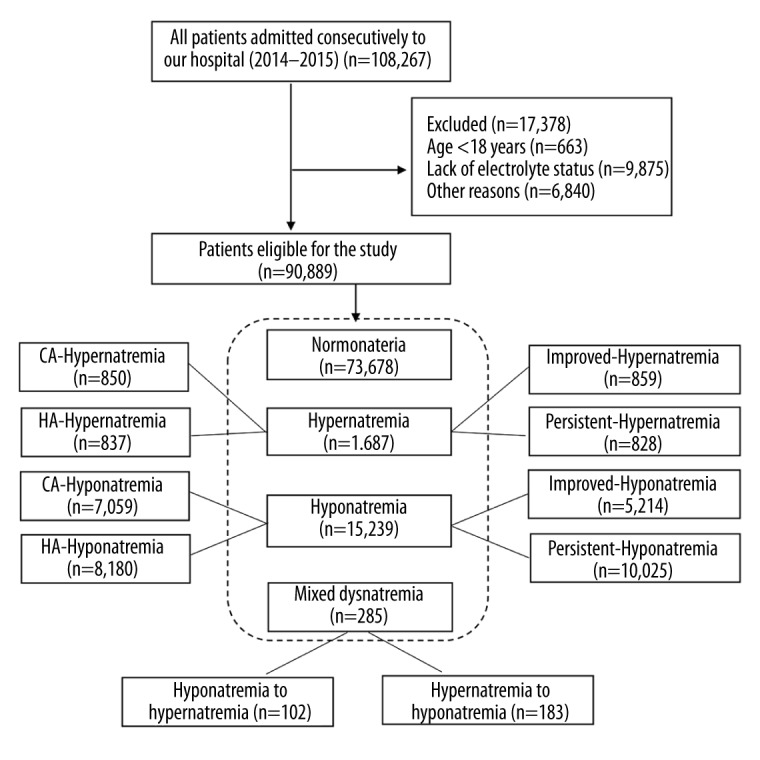
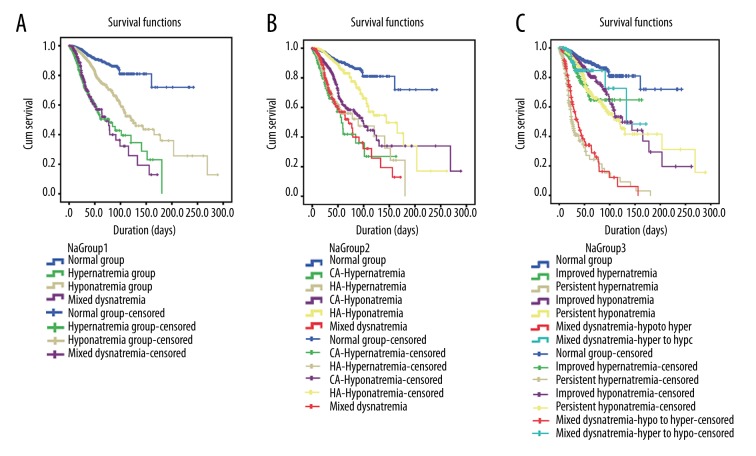
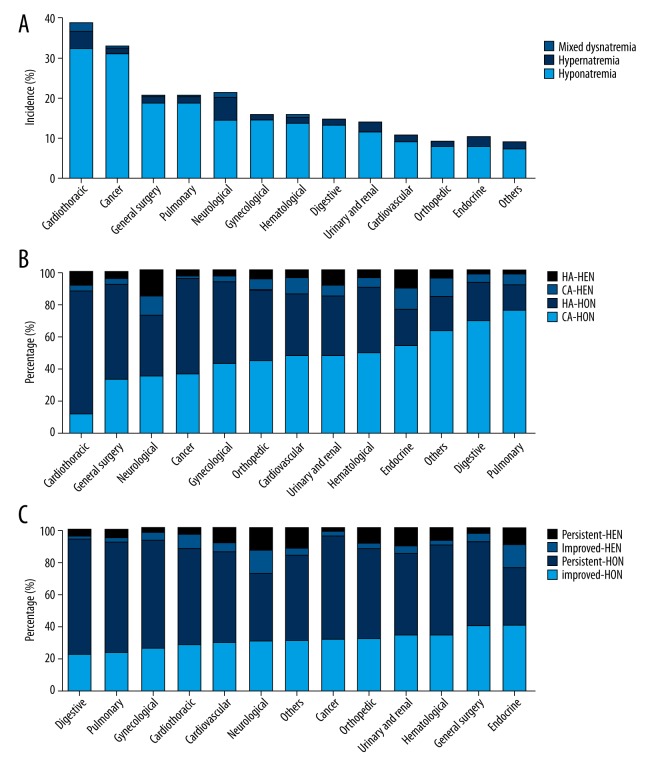
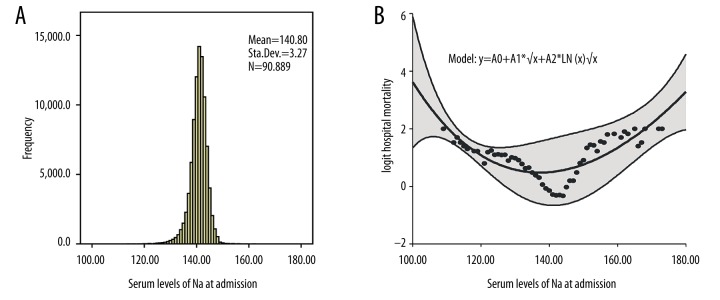
本研究共纳入90889例患者。根据住院期间的血清钠水平,低钠血症和高钠血症的发生率分别为16.8%和1.9%。混合性钠代谢紊乱(定义为同一患者在住院期间同时发生低钠血症和高钠血症)的发生率为0.3%。不同基础疾病中钠代谢紊乱的发生率不同。多项逻辑回归分析显示,各种钠代谢紊乱均与医院死亡率独立相关。以下钠代谢紊乱是医院死亡率的强预测因素:混合性钠代谢紊乱(比值比22.344,95%可信区间15.709 - 31.783,P = 0.000)、高钠血症(比值比13.387,95%可信区间10.642 - 16.840,P = 0.000),尤其是医院获得性(比值比16.216,95%可信区间12.588 - 20.888,P = 0.000)和持续性(比值比22.983,95%可信区间17.554 - 30.092,P = 0.000)高钠血症。低钠血症也是医院死亡率的一个危险因素(比值比2.225,95%可信区间1.857 - 2.667)。然而,如果低钠血症过度纠正为高钠血症,比值比则升至56.884(95%可信区间35.098 - 92.193)。
钠代谢紊乱与不良预后独立相关。医院获得性和持续性高钠血症是医院死亡率的强危险因素。对高危患者有效预防和适当纠正钠代谢紊乱可能会降低医院死亡率。