Biomedical Informatics and Public Health Department, Hôpital Européen G. Pompidou, Assistance Publique-Hôpitaux de Paris, Paris, France.
Sorbonne Universités, UPMC Univ Paris 06, UMR_S 1138, Centre de Recherche des Cordeliers, F-75006, Paris, France.
BMC Med Inform Decis Mak. 2017 Nov 22;17(1):152. doi: 10.1186/s12911-017-0549-7.
Even small variations of serum sodium concentration may be associated with mortality. Our objective was to confirm the impact of borderline dysnatremia for patients admitted to hospital on in-hospital mortality using real life care data from our electronic health record (EHR) and a phenome-wide association analysis (PheWAS).
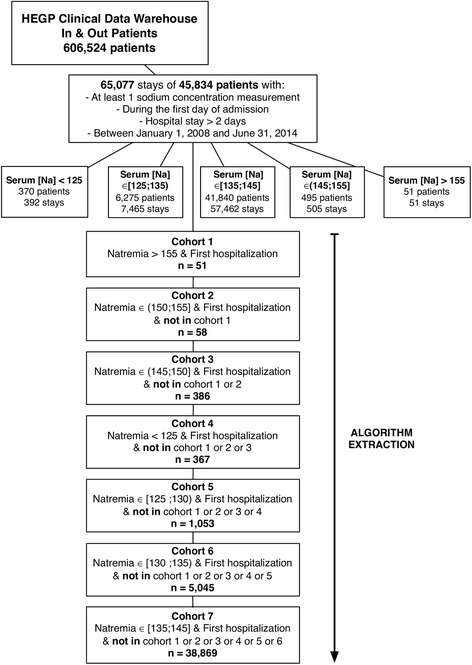
Retrospective observational study based on patient data admitted to Hôpital Européen George Pompidou, between 01/01/2008 and 31/06/2014; including 45,834 patients with serum sodium determinations on admission. We analyzed the association between dysnatremia and in-hospital mortality, using a multivariate logistic regression model to adjust for classical potential confounders. We performed a PheWAS to identify new potential confounders.
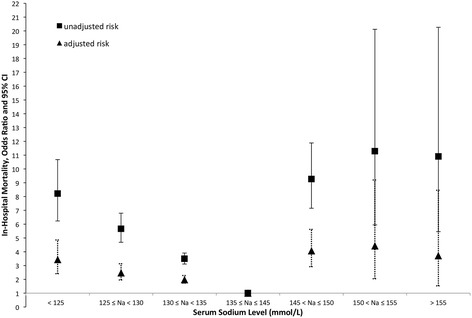
Hyponatremia and hypernatremia were recorded for 12.0% and 1.0% of hospital stays, respectively. Adjusted odds ratios (ORa) for severe, moderate and borderline hyponatremia were 3.44 (95% CI, 2.41-4.86), 2.48 (95% CI, 1.96-3.13) and 1.98 (95% CI, 1.73-2.28), respectively. ORa for severe, moderate and borderline hypernatremia were 4.07 (95% CI, 2.92-5.62), 4.42 (95% CI, 2.04-9.20) and 3.72 (95% CI, 1.53-8.45), respectively. Borderline hyponatremia (ORa = 1.57 95% CI, 1.35-1.81) and borderline hypernatremia (ORa = 3.47 95% CI, 2.43-4.90) were still associated with in-hospital mortality after adjustment for classical and new confounding factors identified through the PheWAS analysis.
Borderline dysnatremia on admission are independently associated with a higher risk of in-hospital mortality. By using medical data automatically collected in EHR and a new data mining approach, we identified new potential confounding factors that were highly associated with both mortality and dysnatremia.
血清钠浓度的微小变化也可能与死亡率相关。我们的目的是使用来自电子健康记录 (EHR) 的真实护理数据和表型全基因组关联分析 (PheWAS),确认入院患者边界性电解质紊乱对住院死亡率的影响。
基于 2008 年 1 月 1 日至 2014 年 6 月 31 日期间在 Hôpital Européen George Pompidou 住院的患者数据进行回顾性观察性研究,共纳入 45834 例入院时测定血清钠的患者。我们使用多变量逻辑回归模型来调整经典潜在混杂因素,分析电解质紊乱与住院死亡率之间的关系。我们进行了表型全基因组关联分析,以确定新的潜在混杂因素。
低钠血症和高钠血症的住院记录分别为 12.0%和 1.0%。严重、中度和轻度低钠血症的校正比值比 (ORa) 分别为 3.44 (95%CI, 2.41-4.86)、2.48 (95%CI, 1.96-3.13) 和 1.98 (95%CI, 1.73-2.28)。严重、中度和轻度高钠血症的校正比值比 (ORa) 分别为 4.07 (95%CI, 2.92-5.62)、4.42 (95%CI, 2.04-9.20) 和 3.72 (95%CI, 1.53-8.45)。校正经典和通过表型全基因组关联分析确定的新混杂因素后,轻度低钠血症 (ORa=1.57,95%CI,1.35-1.81) 和轻度高钠血症 (ORa=3.47,95%CI,2.43-4.90) 仍与住院死亡率相关。
入院时的边界性电解质紊乱与住院死亡率的升高独立相关。通过使用 EHR 自动收集的医疗数据和新的数据挖掘方法,我们确定了与死亡率和电解质紊乱高度相关的新潜在混杂因素。