Soliman Pamela T, Westin Shannon N, Dioun Shayan, Sun Charlotte C, Euscher Elizabeth, Munsell Mark F, Fleming Nicole D, Levenback Charles, Frumovitz Michael, Ramirez Pedro T, Lu Karen H
Department of Gynecologic Oncology and Reproductive Medicine, University of Texas, M.D. Anderson Cancer Center, Houston, TX, United States.
Department of Gynecologic Oncology and Reproductive Medicine, University of Texas, M.D. Anderson Cancer Center, Houston, TX, United States.
Gynecol Oncol. 2017 Aug;146(2):234-239. doi: 10.1016/j.ygyno.2017.05.016. Epub 2017 May 18.
Sentinel lymph node (SLN) mapping continues to evolve in the surgical staging of endometrial cancer (EC). The purpose of this trial was to identify the sensitivity, false negative rate (FNR) and FN predictive value (FNPV) of SLN compared to complete pelvic and para-aortic lymphadenectomy (LAD) in women with high-risk EC.
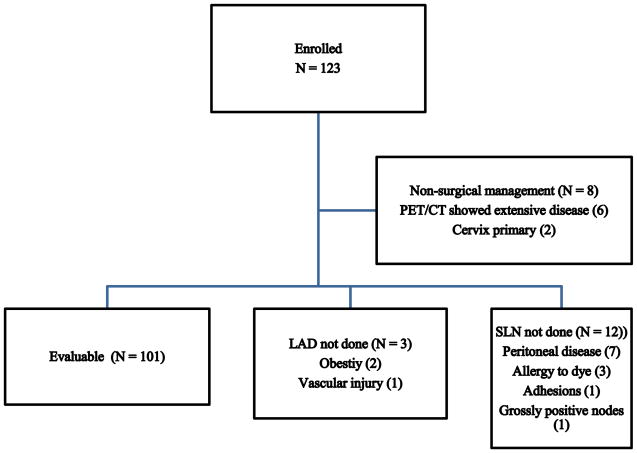
Women with high-risk EC (grade 3, serous, clear cell, carcinosarcoma) were enrolled in this prospective surgical trial. All patients underwent preoperative PET/CT and intraoperative SLN biopsy followed by LAD. Patients with peritoneal disease on imaging or at the time of surgery were excluded. Patients were evaluable if SLN was attempted and complete LAD was performed.
123 patients were enrolled between 4/13 and 5/16; 101 were evaluable. At least 1 SLN was identified in 89% (90); bilateral detection 58%, unilateral pelvic 40%, para-aortic only 2%. Indocyanine green was used in 61%, blue dye in 28%, and blue dye and technetium in 11%. Twenty-three pts. (23%) had ≥1 positive node. In 20/23, ≥1 SLN was identified and in 19/20 the SLN was positive. Only 1 patient had bilateral negative SLN and positive non-SLNs on final pathology. Overall, sensitivity of SLN was 95% (19/20), FNR was 5% (1/20) and FNPV was 1.4% (1/71). If side-specific LAD was performed when a SLN was not detected, the FNR decreased to 4.3% (1/23).
This prospective trial demonstrated that SLN biopsy plus side-specific LAD, when SLN is not detected, is a reasonable alternative to a complete LAD in high-risk endometrial cancer.
前哨淋巴结(SLN)图谱在子宫内膜癌(EC)手术分期中的应用仍在不断发展。本试验的目的是确定高危EC女性中SLN与盆腔和腹主动脉旁淋巴结完全切除术(LAD)相比的敏感性、假阴性率(FNR)和FN预测值(FNPV)。
高危EC(3级、浆液性、透明细胞、癌肉瘤)女性纳入本前瞻性手术试验。所有患者术前行PET/CT检查及术中SLN活检,随后行LAD。影像检查或手术时发现有腹膜疾病的患者被排除。若尝试进行SLN活检且完成LAD,则患者可进行评估。
2013年4月至2016年5月期间共纳入123例患者;101例可进行评估。89%(90例)患者至少识别出1个SLN;双侧检测率为58%,单侧盆腔检测率为40%,仅腹主动脉旁检测率为2%。61%的患者使用了吲哚菁绿,28%使用了蓝色染料,11%使用了蓝色染料和锝。23例患者(23%)有≥1个阳性淋巴结。在23例中的20例中,识别出≥1个SLN,其中19/20的SLN为阳性。最终病理检查仅1例患者双侧SLN阴性但非SLN阳性。总体而言,SLN的敏感性为95%(19/20),FNR为5%(1/20),FNPV为1.4%(1/71)。若未检测到SLN时进行侧方特异性LAD,FNR降至4.3%(1/23)。
这项前瞻性试验表明,对于高危子宫内膜癌,SLN活检加侧方特异性LAD(当未检测到SLN时)是完全LAD的合理替代方案。