Srinivasan Mukund, Kamath Padmanabh, Bhat Narayan, Pai Narasimha, Bhat Rajesh, Shah Tejas, Manjrekar Poornima, Mahabala Chakrapani
Department of Internal Medicine, Kasturba Medical College, Manipal University, Mangalore, Karnataka 575001 India.
Department of Cardiology, Kasturba Medical College, Manipal University, Mangalore, Karnataka India.
Diabetol Metab Syndr. 2017 May 19;9:38. doi: 10.1186/s13098-017-0237-x. eCollection 2017.
There is a substantial reduction in cardiovascular related morbidity and mortality in the general population attributed to improved treatment of cardiac risk factors and disease, the same magnitude of benefit has not been observed in those with diabetes mellitus. The aim of the present study was to evaluate factors associated with the cardiac outcome at 1 year after coronary angiogram in patients with type 2 diabetes mellitus and to compare the outcomes with nondiabetics.
A retrospective cohort study was carried out in subjects who underwent coronary angiogram for an evaluation of CAD, with follow-up data available for period of 12 months. The data consisted of 208 type 2 diabetic and 75 non-diabetic patients. Clinical, anthropometric and other biochemical risk factors of the study participants were recorded. Univariate and multivariate cox proportional hazard regression analyses were performed to evaluate the relation between the cardiovascular risk factors and major adverse cardiac events (MACE).
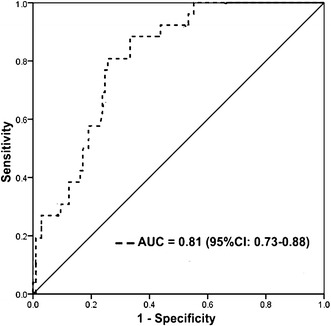
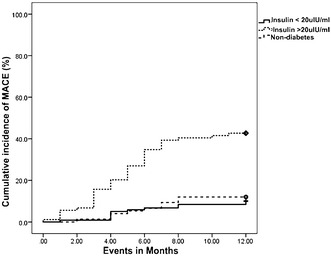
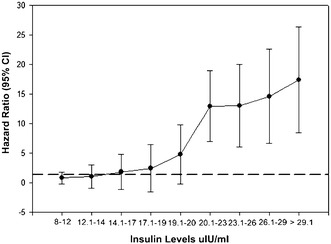
At 1 year, MACE was observed in 50 (24.04%) type 2 diabetic subjects, which included non-fatal myocardial infarction 24 (11.54%), target vessel revascularization 15 (7.21%) and death 11 (5.29%). The area under the curve for insulin in predicting MACE was found to be 0.81 (95% CI 0.73-0.88) with sensitivity and specificity of 88% (95% CI 0.71-0.96) and 74% (95% CI 0.65-0.81) respectively. After adjustment for potential confounders hyperinsulinemia (>20 µIU/ml) was significantly associated with MACE [adjusted hazard ratio (HR): 3.03, 95% CI 1.41-6.54, p = 0.005]. Interestingly, the MACE rate in type 2 diabetics with insulin levels <20 µIU/ml (10.2%) and non-diabetics (12%) (p = 0.676) appears to be same.
In addition to severity of the CAD at the baseline, basal hyperinsulinemia beyond a threshold strongly predicts adverse cardiac events at 1 year in type 2 diabetes mellitus. Those below the threshold, appears to be having a risk equivalent to non-diabetics.
由于心脏危险因素和疾病的治疗得到改善,普通人群中心血管相关发病率和死亡率大幅降低,但在糖尿病患者中尚未观察到同等程度的益处。本研究的目的是评估2型糖尿病患者冠状动脉造影后1年与心脏结局相关的因素,并将结果与非糖尿病患者进行比较。
对因评估冠心病而接受冠状动脉造影的受试者进行回顾性队列研究,随访数据为期12个月。数据包括208例2型糖尿病患者和75例非糖尿病患者。记录研究参与者的临床、人体测量和其他生化危险因素。进行单因素和多因素Cox比例风险回归分析,以评估心血管危险因素与主要不良心脏事件(MACE)之间的关系。
1年时,50例(24.04%)2型糖尿病受试者发生MACE,其中包括非致命性心肌梗死24例(11.54%)、靶血管血运重建15例(7.21%)和死亡11例(5.29%)。胰岛素预测MACE的曲线下面积为0.81(95%CI 0.73-0.88),敏感性和特异性分别为88%(95%CI 0.71-0.96)和74%(95%CI 0.65-0.81)。在调整潜在混杂因素后,高胰岛素血症(>20 μIU/ml)与MACE显著相关[调整后风险比(HR):3.03,95%CI 1.41-6.54,p = 0.005]。有趣的是,胰岛素水平<20 μIU/ml的2型糖尿病患者(10.2%)和非糖尿病患者(12%)的MACE发生率似乎相同(p = 0.676)。
除了基线时冠心病的严重程度外,超过阈值的基础高胰岛素血症强烈预测2型糖尿病患者1年时的不良心脏事件。低于阈值的患者,其风险似乎与非糖尿病患者相当。