Sudre Carole H, Bocchetta Martina, Cash David, Thomas David L, Woollacott Ione, Dick Katrina M, van Swieten John, Borroni Barbara, Galimberti Daniela, Masellis Mario, Tartaglia Maria Carmela, Rowe James B, Graff Caroline, Tagliavini Fabrizio, Frisoni Giovanni, Laforce Robert, Finger Elizabeth, de Mendonça Alexandre, Sorbi Sandro, Ourselin Sébastien, Cardoso M Jorge, Rohrer Jonathan D
Dementia Research Centre, Department of Neurodegenerative Disease, UCL Institute of Neurology, Queen Square, London, UK; Centre for Medical Image Computing, University College London, UK.
Dementia Research Centre, Department of Neurodegenerative Disease, UCL Institute of Neurology, Queen Square, London, UK.
Neuroimage Clin. 2017 Apr 26;15:171-180. doi: 10.1016/j.nicl.2017.04.015. eCollection 2017.
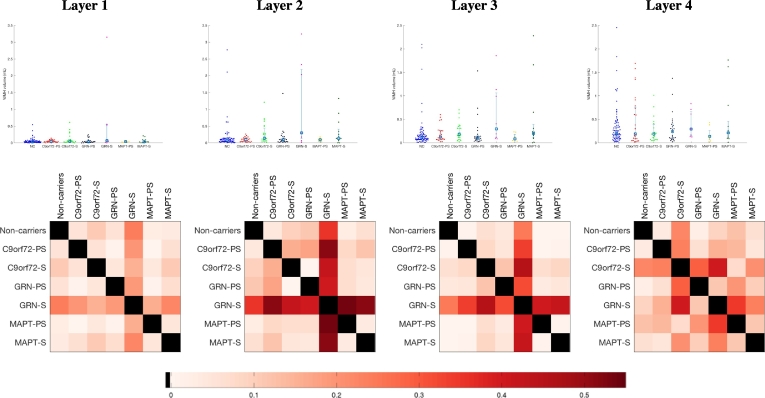
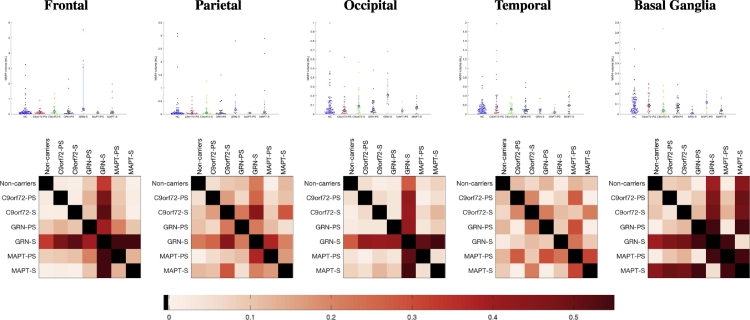
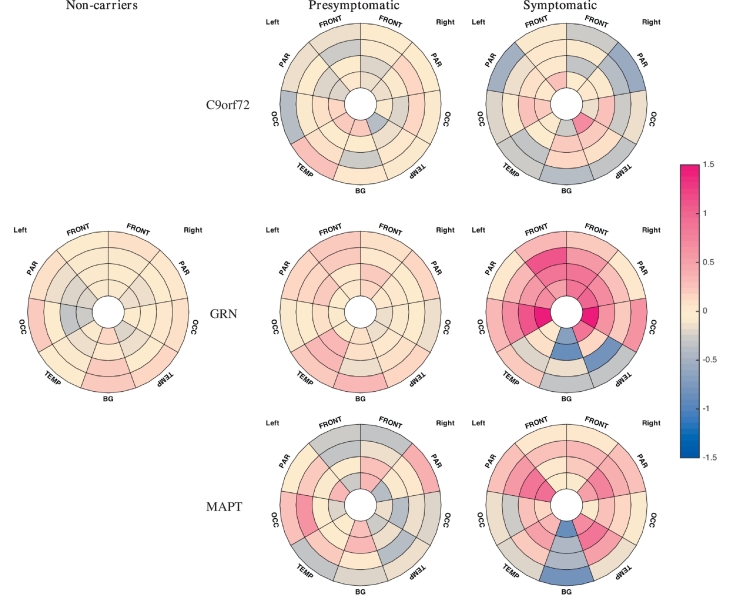
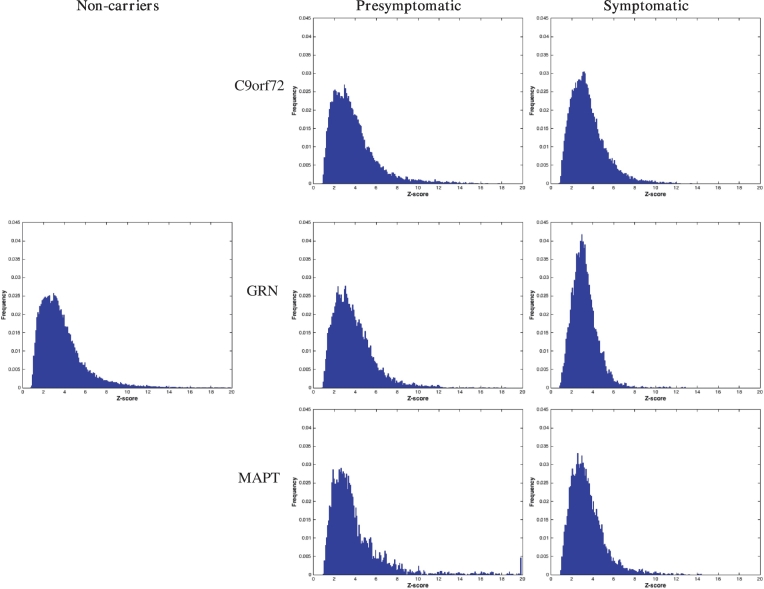
Genetic frontotemporal dementia is most commonly caused by mutations in the progranulin , microtubule-associated protein tau ( and chromosome 9 open reading frame 72 ) genes. Previous small studies have reported the presence of cerebral white matter hyperintensities (WMH) in genetic FTD but this has not been systematically studied across the different mutations. In this study WMH were assessed in 180 participants from the Genetic FTD Initiative (GENFI) with 3D T1- and T2-weighed magnetic resonance images: 43 symptomatic (7 , 13 and 23 ), 61 presymptomatic mutation carriers (25 , 8 and 28 ) and 76 mutation negative non-carrier family members. An automatic detection and quantification algorithm was developed for determining load, location and appearance of WMH. Significant differences were seen only in the symptomatic group compared with the other groups with no differences in the or groups: increased global load of WMH was seen, with WMH located in the frontal and occipital lobes more so than the parietal lobes, and nearer to the ventricles rather than juxtacortical. Although no differences were seen in the presymptomatic group as a whole, in the cohort only there was an association of increased WMH volume with expected years from symptom onset. The appearance of the WMH was also different in the group compared with the other groups, with the lesions in the group being more similar to each other. The presence of WMH in those with progranulin deficiency may be related to the known role of progranulin in neuroinflammation, although other roles are also proposed including an effect on blood-brain barrier permeability and the cerebral vasculature. Future studies will be useful to investigate the longitudinal evolution of WMH and their potential use as a biomarker as well as post-mortem studies investigating the histopathological nature of the lesions.
遗传性额颞叶痴呆最常见的病因是原纤维蛋白、微管相关蛋白tau(以及9号染色体开放阅读框72)基因的突变。先前的小型研究报告了遗传性额颞叶痴呆中存在脑白质高信号(WMH),但尚未针对不同突变进行系统研究。在本研究中,利用三维T1加权和T2加权磁共振成像对来自遗传性额颞叶痴呆倡议组织(GENFI)的180名参与者的WMH进行了评估:43名有症状者(分别为7名、13名和23名)、61名症状前突变携带者(分别为25名、8名和28名)以及76名突变阴性的非携带者家庭成员。开发了一种自动检测和量化算法,用于确定WMH的负荷、位置和外观。仅在有症状组与其他组之间观察到显著差异,而在或组之间无差异:WMH的整体负荷增加,WMH位于额叶和枕叶的情况比顶叶更多,且更靠近脑室而非皮质下。虽然在症状前组整体未观察到差异,但仅在队列中,WMH体积增加与距症状出现的预期年数之间存在关联。与其他组相比,组中WMH的外观也有所不同,组中的病变彼此更相似。原纤维蛋白缺乏者中WMH的存在可能与原纤维蛋白在神经炎症中的已知作用有关,尽管也提出了其他作用,包括对血脑屏障通透性和脑血管系统的影响。未来的研究将有助于调查WMH的纵向演变及其作为生物标志物的潜在用途,以及对病变组织病理学性质进行尸检研究。