School of Public Health, Peking University, Xueyuan Road 38#, Beijing, 100191, China.
London School of Hygiene and Tropical Medicine, London, UK.
Int J Equity Health. 2017 May 23;16(1):49. doi: 10.1186/s12939-017-0541-y.
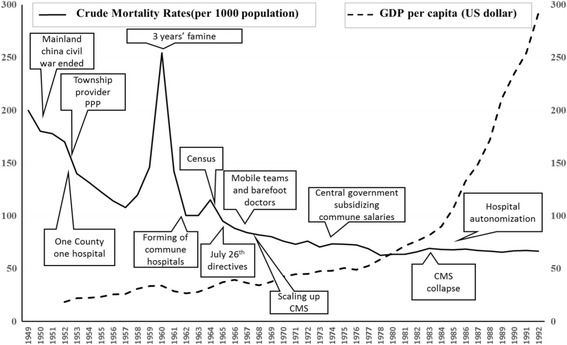
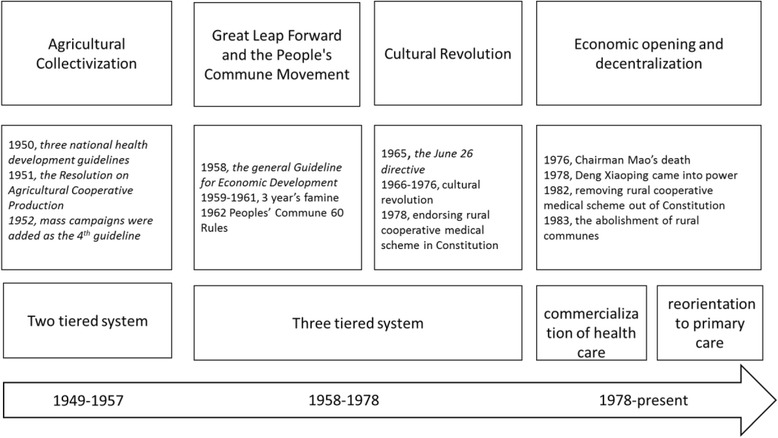
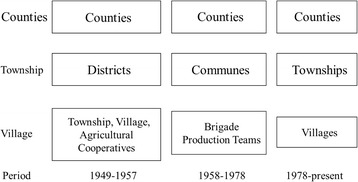
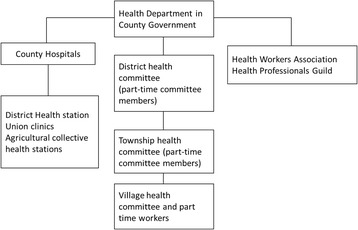
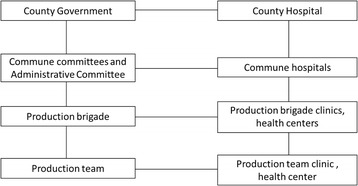
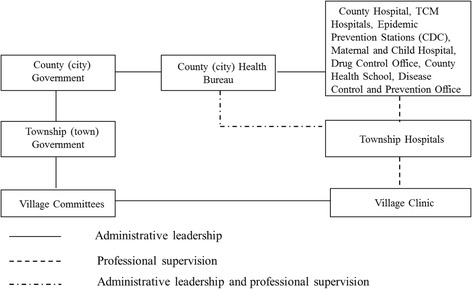
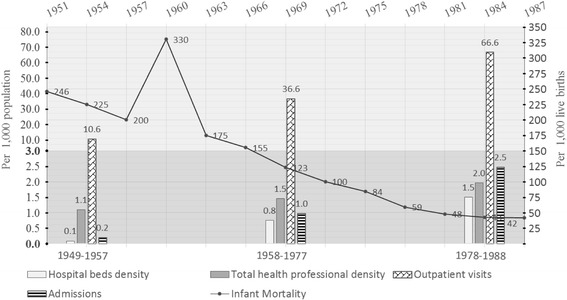
China has made remarkable progress in scaling up essential services during the last six decades, making health care increasingly available in rural areas. This was partly achieved through the building of a three-tier health system in the 1950s, established as a linked network with health service facilities at county, township and village level, to extend services to the whole population.
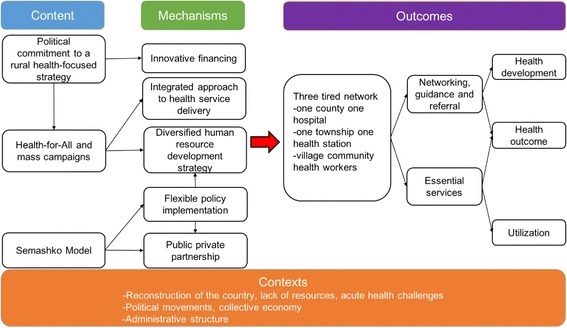
We developed a Theory of Change to chart the policy context, contents and mechanisms that may have facilitated the establishment of the three-tier health service delivery system in rural China. We systematically synthesized the best available evidence on how China achieved universal access to essential services in resource-scarce rural settings, with a particular emphasis on the experiences learned before the 1980s, when the country suffered a particularly acute lack of resources.
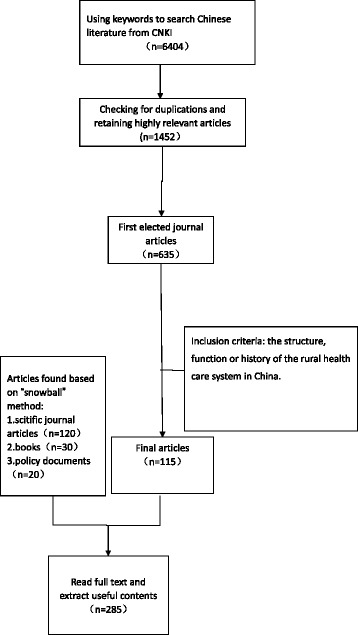
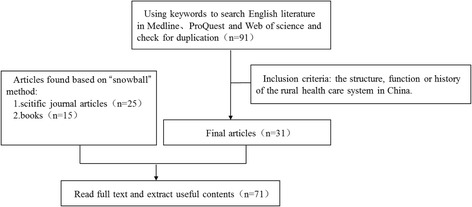
The search identified only three peered-reviewed articles that fit our criteria for scientific rigor. We therefore drew extensively on government policy documents, and triangulated them with other publications and key informant interviews. We found that China's three-tier health service delivery system was established in response to acute health challenges, including high fertility and mortality rates. Health system resources were extremely low in view of the needs and insufficient to extend access to even basic care. With strong political commitment to rural health and a "health-for-all" policy vision underlying implementation, a three-tier health service delivery model connecting villages, townships and counties was quickly established. We identified several factors that contributed to the success of the three-tier system in China: a realistic health human resource development strategy, use of mass campaigns as a vehicle to increase demand, an innovative financing mechanisms, public-private partnership models in the early stages of scale up, and an integrated approach to service delivery. An implementation process involving gradual adaptation and incorporation of the lessons learnt was also essential.
China's 60 year experience in establishing a de-professionalized, community-based, health service delivery model that is economically feasible, institutionally and culturally appropriate mechanism can be useful to other low- and middle-income countries (LMICs) seeking to extend essential services. Lessons can be drawn from both reform content and from its implementation pathway, identifying the political, institutional and contextual factors shaping the three-tier delivery model over time.
中国在过去六十年中在扩大基本服务方面取得了显著进展,使农村地区的医疗保健服务越来越普及。这在一定程度上是通过在 20 世纪 50 年代建立三级卫生系统实现的,该系统建立了一个县、乡和村各级卫生服务设施相连的网络,将服务扩展到全体人民。
我们制定了一个变革理论,以描绘政策背景、内容和机制,这些可能有助于在中国农村建立三级卫生服务提供系统。我们系统地综合了有关中国如何在资源匮乏的农村环境中实现基本服务普及的最佳现有证据,特别强调了 20 世纪 80 年代以前的经验,当时该国特别缺乏资源。
搜索仅确定了符合我们科学严谨性标准的三篇同行评审文章。因此,我们广泛借鉴了政府政策文件,并将其与其他出版物和关键知情者访谈进行了三角分析。我们发现,中国的三级卫生服务提供系统是为应对包括高生育率和死亡率在内的急性健康挑战而建立的。鉴于需求极低,卫生系统资源极为有限,甚至无法提供基本护理。由于对农村卫生的坚定政治承诺和实施“人人享有健康”政策愿景,一个连接村庄、乡镇和县城的三级卫生服务提供模式迅速建立起来。我们确定了几个有助于中国三级系统成功的因素:现实的卫生人力资源开发战略、利用群众运动作为增加需求的手段、创新的融资机制、在规模化的早期阶段公私伙伴关系模式,以及服务提供的综合方法。实施过程中涉及逐步适应和纳入经验教训也是至关重要的。
中国在过去 60 年中建立了一个去专业化、以社区为基础、经济可行、机构和文化上合适的卫生服务提供模式的经验,对于其他寻求扩大基本服务的中低收入国家(LMICs)可能是有用的。可以从改革内容和实施途径中吸取教训,确定随着时间的推移塑造三级交付模式的政治、制度和背景因素。