School of Medicine and Health Management, Tongji Medical College, Huazhong University of Science and Technology, No 13 Hangkong Road, Qiaokou District Wuhan, Hubei, 430030, China.
Department of Medical Affairs, Guangdong General Hospital, Guangzhou, 510080, Guangdong, China.
Int J Equity Health. 2018 May 2;17(1):55. doi: 10.1186/s12939-018-0766-4.
China's rapid transition in healthcare service system has posed considerable challenges for the primary care system. Little is known regarding the capacity of township hospitals (THs) to deliver surgical care in rural China with over 600 million lives. We aimed to ascertain its current performance, barriers, and summary lessons for its re-building in central China.
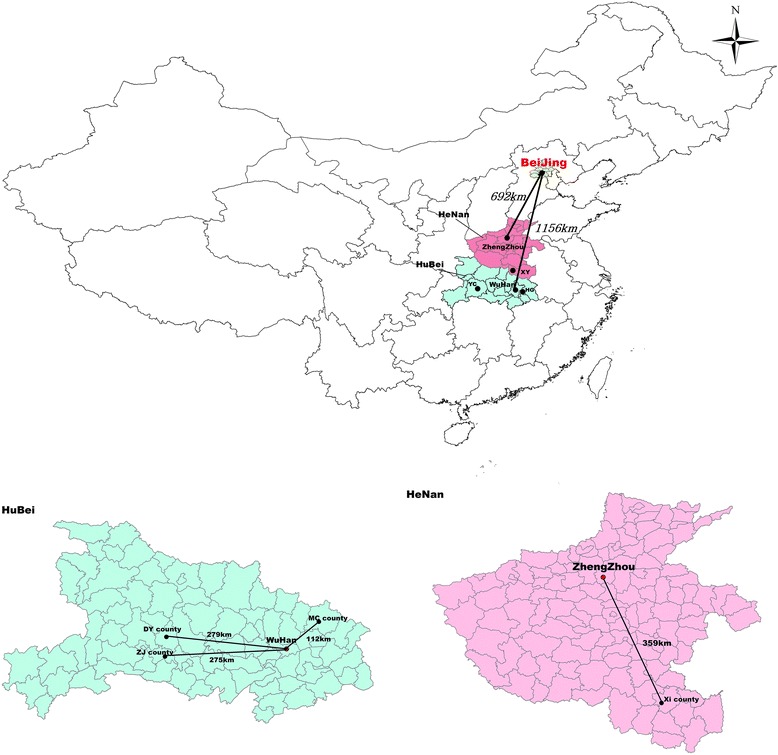
This study was conducted in four counties from two provinces in central China. The New Rural Cooperative Medical System (NRCMS) claim data from two counties in Hubei province was analyzed to describe the current situation of surgical care provision. Based on previous studies, self-administered questionnaire was established to collect key indicators from 60 THs from 2011 to 2015, and social and economic statuses of the sampling townships were collected from the local statistical yearbook. Semi-structured interviews were conducted among seven key administrators in the THs that did not provide appendectomy care in 2015. Determinants of appendectomy care provision were examined using a negative binominal regression model.
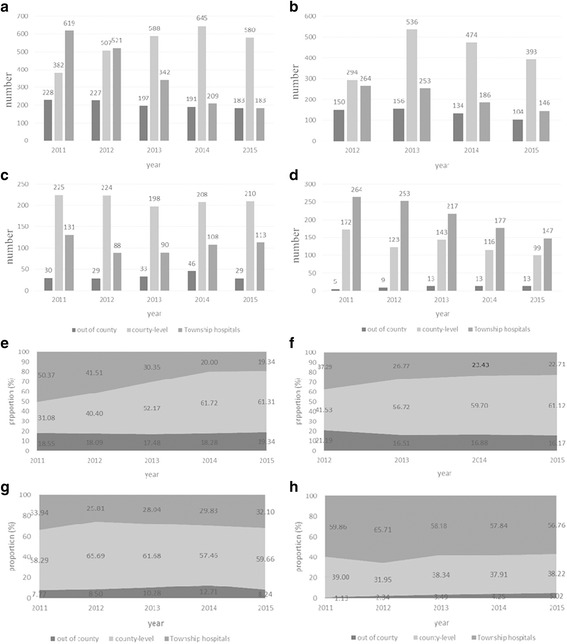
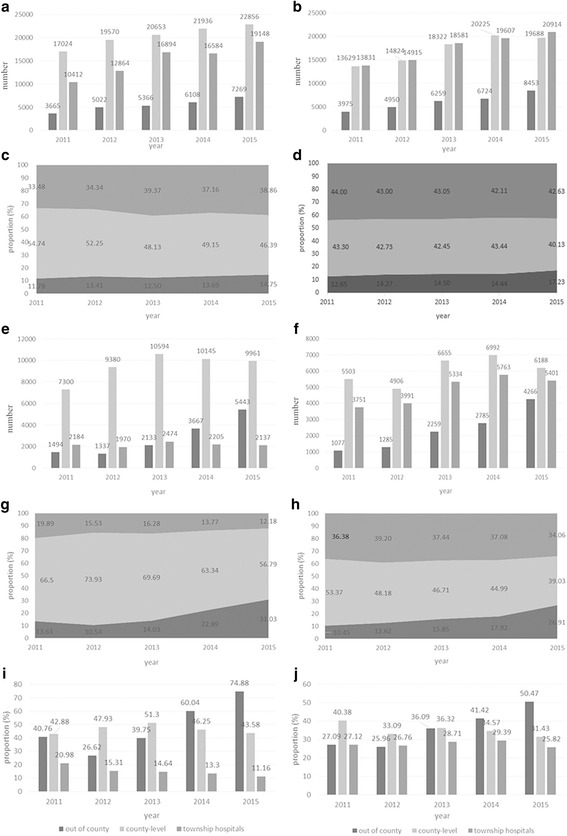
First, with the rapid increase in inpatient services provided by the THs, their proportion of surgical service provision has been nibbled by out-of-county facilities. Second, although DY achieved a stable performance, the total amount of appendectomy provided by the 60 THs decreased to 589 in 2015 from 1389 in 2011. Moreover, their proportion reduced to 26.77% in 2015 from 41.84% in 2012. Third, an increasing number of THs did not provide appendectomy in 2015, with the shortage of anesthesiologists and equipment as the most mentioned reasons (46.43%). Estimation results from the negative binomial model indicated that the annual average per capita disposable income and tightly integrated delivery networks (IDNs) negatively affected the amount of appendectomy provided by THs. By contrast, the probability of appendectomy provision by THs was increased by performance-related payment (PRP). Out-of-pocket (OOP) cost gap of appendectomy services between the two different levels of facilities, payment method, and the size of THs presented no observable improvement to the likelihood of appendectomy care in THs.
The county-level health system did not effectively respond to the continuously increasing surgical care need. The surgical capacity of THs declined with the surgical patterns' simplistic and quantity reduction. Deficits and critical challenges for surgical capacity building in central China were identified, including shortage of human resources and medical equipment and increasing income. Moreover, tight IDNs do not temporarily achieve capacity building. Therefore, the reimbursement rate should be further ranged, and physicians should be incentivized appropriately. The administrators, policy makers, and medical staff of THs should be aware of these findings owing to the potential benefits for the capacity building of the rural healthcare system.
中国医疗服务体系的快速转型给基层医疗体系带来了相当大的挑战。对于拥有超过 6 亿人口的中国农村地区的乡镇卫生院(THs)提供外科护理的能力,人们知之甚少。我们旨在确定其目前在中部地区的重建表现、障碍和总结经验。
本研究在中部两个省份的四个县进行。对湖北省两个县的新型农村合作医疗(NRCMS)报销数据进行了分析,以描述外科护理提供的现状。根据以往的研究,我们从 2011 年到 2015 年建立了一个自我管理的问卷,以收集 60 家 TH 的关键指标,并从当地统计年鉴中收集了抽样乡镇的社会和经济状况。对 2015 年不提供阑尾切除术的 7 家 TH 关键管理人员进行了半结构化访谈。使用负二项回归模型检查阑尾切除术提供的决定因素。
首先,随着 THs 提供的住院服务的快速增加,其外科服务提供的比例已被县外医疗机构蚕食。其次,尽管 DY 表现稳定,但 60 家 THs 提供的阑尾切除术总量从 2011 年的 1389 例下降到 2015 年的 589 例。此外,其比例从 2012 年的 41.84%降至 2015 年的 26.77%。第三,越来越多的 THs 在 2015 年不再提供阑尾切除术,麻醉师和设备短缺是最常提到的原因(46.43%)。负二项模型的估计结果表明,人均可支配收入和紧密整合的交付网络(IDNs)每年都会对 THs 提供的阑尾切除术数量产生负面影响。相比之下,绩效相关支付(PRP)增加了 THs 提供阑尾切除术的可能性。来自不同级别设施、支付方式和 THs 规模的阑尾切除术服务的自付费用差距并没有观察到对 THs 阑尾切除术护理可能性的改善。
县级卫生系统未能有效应对不断增加的外科护理需求。THs 的外科能力随着外科模式的简化和数量减少而下降。确定了中部地区外科能力建设的缺陷和关键挑战,包括人力资源和医疗设备短缺以及收入增加。此外,紧密的 IDNs 暂时无法实现能力建设。因此,报销率应进一步扩大,应适当激励医生。THs 的管理人员、政策制定者和医务人员应意识到这些发现,因为这对农村医疗体系的能力建设可能带来潜在的好处。