Giattino Charles M, Gardner Jacob E, Sbahi Faris M, Roberts Kenneth C, Cooter Mary, Moretti Eugene, Browndyke Jeffrey N, Mathew Joseph P, Woldorff Marty G, Berger Miles
Center for Cognitive Neuroscience, Duke UniversityDurham, NC, USA.
Department of Psychology and Neuroscience, Duke UniversityDurham, NC, USA.
Front Syst Neurosci. 2017 May 8;11:24. doi: 10.3389/fnsys.2017.00024. eCollection 2017.
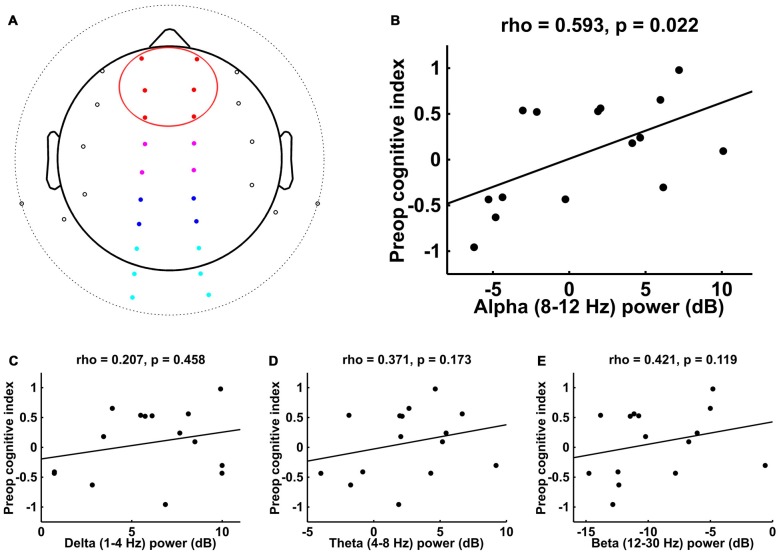
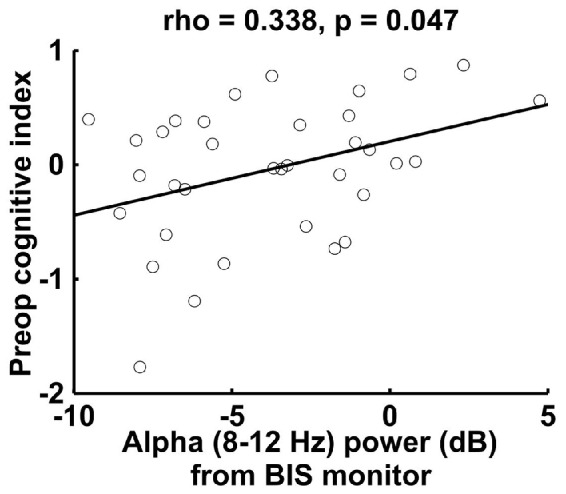
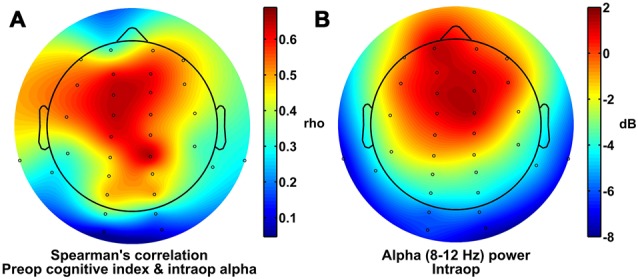
Each year over 16 million older Americans undergo general anesthesia for surgery, and up to 40% develop postoperative delirium and/or cognitive dysfunction (POCD). Delirium and POCD are each associated with decreased quality of life, early retirement, increased 1-year mortality, and long-term cognitive decline. Multiple investigators have thus suggested that anesthesia and surgery place severe stress on the aging brain, and that patients with less ability to withstand this stress will be at increased risk for developing postoperative delirium and POCD. Delirium and POCD risk are increased in patients with lower preoperative cognitive function, yet preoperative cognitive function is not routinely assessed, and no intraoperative physiological predictors have been found that correlate with lower preoperative cognitive function. Since general anesthesia causes alpha-band (8-12 Hz) electroencephalogram (EEG) power to decrease occipitally and increase frontally (known as "anteriorization"), and anesthetic-induced frontal alpha power is reduced in older adults, we hypothesized that lower intraoperative frontal alpha power might correlate with lower preoperative cognitive function. Here, we provide evidence that such a correlation exists, suggesting that lower intraoperative frontal alpha power could be used as a physiological marker to identify older adults with lower preoperative cognitive function. Lower intraoperative frontal alpha power could thus be used to target these at-risk patients for possible therapeutic interventions to help prevent postoperative delirium and POCD, or for increased postoperative monitoring and follow-up. More generally, these results suggest that understanding interindividual differences in how the brain responds to anesthetic drugs can be used as a probe of neurocognitive function (and dysfunction), and might be a useful measure of neurocognitive function in older adults.
每年有超过1600万美国老年人接受外科手术全身麻醉,其中高达40%的人会出现术后谵妄和/或认知功能障碍(POCD)。谵妄和POCD均与生活质量下降、提前退休、1年死亡率增加以及长期认知衰退有关。因此,多位研究人员认为,麻醉和手术会给衰老的大脑带来巨大压力,而承受这种压力能力较弱的患者发生术后谵妄和POCD的风险会增加。术前认知功能较低的患者发生谵妄和POCD的风险会增加,但术前认知功能并未常规评估,而且尚未发现与术前认知功能较低相关的术中生理预测指标。由于全身麻醉会导致枕叶的α波段(8 - 12赫兹)脑电图(EEG)功率降低,额叶功率增加(称为“额叶化”),并且老年人麻醉诱导的额叶α功率会降低,我们推测术中较低的额叶α功率可能与较低的术前认知功能相关。在此,我们提供证据表明这种相关性确实存在,这表明术中较低的额叶α功率可作为一种生理标志物,用于识别术前认知功能较低的老年人。因此,术中较低的额叶α功率可用于针对这些高危患者进行可能的治疗干预,以帮助预防术后谵妄和POCD,或加强术后监测及随访。更一般地说,这些结果表明,了解大脑对麻醉药物反应的个体差异可作为神经认知功能(及功能障碍)的一种探究手段,并且可能是评估老年人神经认知功能的一种有用方法。