Ning Matthew, Rodionov Andrei, Ross Jessica M, Ozdemir Recep A, Burch Maja, Lian Shu Jing, Alsop David, Cavallari Michele, Dickerson Bradford C, Fong Tamara G, Jones Richard N, Libermann Towia A, Marcantonio Edward R, Santarnecchi Emiliano, Schmitt Eva M, Touroutoglou Alexandra, Travison Thomas G, Acker Leah, Reese Melody, Sun Haoqi, Westover Brandon, Berger Miles, Pascual-Leone Alvaro, Inouye Sharon K, Shafi Mouhsin M
Berenson-Allen Center for Noninvasive Brain Stimulation, Beth Israel Deaconess Medical Center, Boston, MA, USA.
BioMag Laboratory, HUS Medical Imaging Center, Helsinki University Hospital, Helsinki, Finland.
medRxiv. 2024 Nov 1:2024.08.15.24312053. doi: 10.1101/2024.08.15.24312053.
Postoperative delirium is the most common complication following surgery among older adults, and has been consistently associated with increased mortality and morbidity, cognitive decline, and loss of independence, as well as markedly increased health-care costs. Electroencephalography (EEG) spectral slowing has frequently been observed during episodes of delirium, whereas intraoperative frontal alpha power is associated with postoperative delirium. We sought to identify preoperative predictors that could identify individuals at high risk for postoperative delirium, which could guide clinical decision-making and enable targeted interventions to potentially decrease delirium incidence and postoperative delirium-related complications.
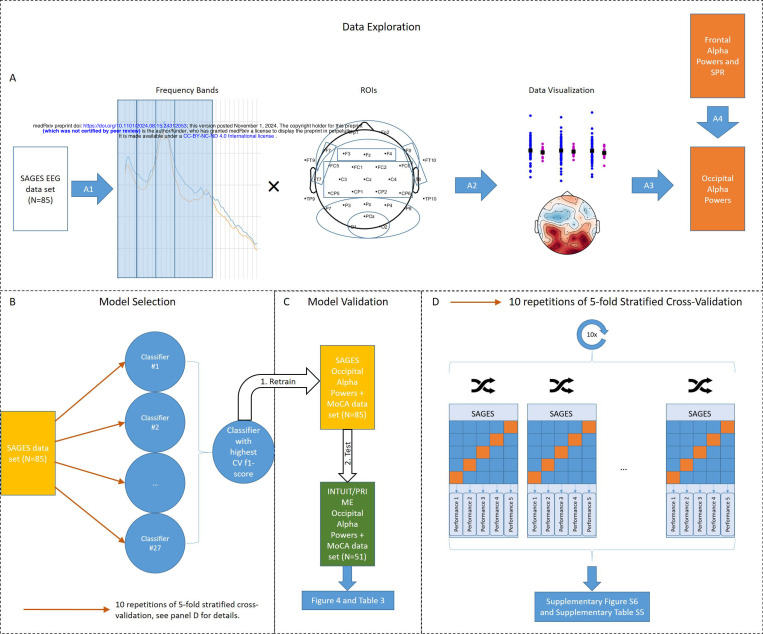
In this prospective observational study, we used machine learning to evaluate whether baseline (preoperative) cognitive function and resting-state EEG could be used to identify patients at risk for postoperative delirium. Preoperative resting-state EEGs and the Montreal Cognitive Assessment were collected from 85 patients (age = 73 ± 6.4 years, 12 cases of delirium) undergoing elective surgery. The model with the highest f1-score was subsequently validated in an independent, prospective cohort of 51 older adults (age = 68 ± 5.2 years, 6 cases of delirium) undergoing elective surgery.
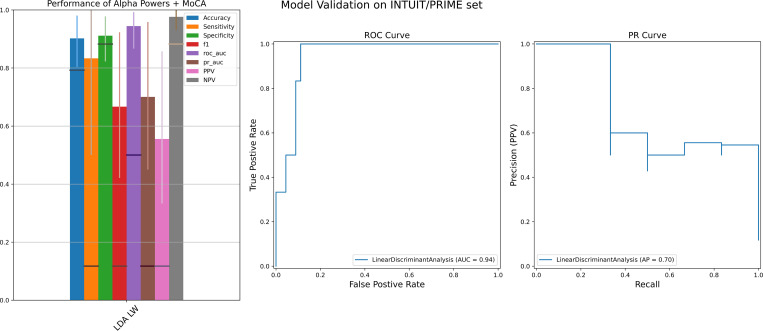
Occipital alpha powers have higher f1-score than frontal alpha powers and EEG spectral slowing in the training cohort. Occipital alpha powers were able to predict postoperative delirium with AUC, specificity and accuracy all >90%, and sensitivity >80%, in the validation cohort. Notably, models incorporating transformed alpha powers and cognitive scores outperformed models incorporating occipital alpha powers alone or cognitive scores alone.
While requiring prospective validation in larger cohorts, these results suggest that strong prediction of postoperative delirium may be feasible in clinical settings using simple and widely available clinical tools. Additionally, our results suggested that the thalamocortical circuit exhibits different EEG patterns under different stressors, with occipital alpha powers potentially reflecting baseline vulnerabilities.
术后谵妄是老年人手术后最常见的并发症,一直与死亡率和发病率增加、认知功能下降、失去独立能力以及医疗保健成本显著增加有关。在谵妄发作期间经常观察到脑电图(EEG)频谱减慢,而术中额叶α波功率与术后谵妄有关。我们试图确定术前预测因素,以识别术后谵妄高危个体,这可以指导临床决策,并进行有针对性的干预,以潜在地降低谵妄发生率和术后谵妄相关并发症。
在这项前瞻性观察研究中,我们使用机器学习来评估基线(术前)认知功能和静息态脑电图是否可用于识别术后谵妄高危患者。收集了85例接受择期手术的患者(年龄=73±6.4岁,12例谵妄)的术前静息态脑电图和蒙特利尔认知评估。随后,在一个由51名接受择期手术的老年人(年龄=68±5.2岁,6例谵妄)组成的独立前瞻性队列中验证了f1分数最高的模型。
在训练队列中,枕叶α波功率的f1分数高于额叶α波功率和脑电图频谱减慢。在验证队列中,枕叶α波功率能够预测术后谵妄,曲线下面积(AUC)、特异性和准确性均>90%,敏感性>80%。值得注意的是,结合转换后的α波功率和认知分数的模型优于仅结合枕叶α波功率或仅结合认知分数的模型。
虽然需要在更大的队列中进行前瞻性验证,但这些结果表明,使用简单且广泛可用的临床工具在临床环境中对术后谵妄进行强有力的预测可能是可行的。此外,我们的结果表明,丘脑皮质回路在不同应激源下表现出不同的脑电图模式,枕叶α波功率可能反映基线易损性。