Baudin Florent, Buisson Alexandra, Vanel Blandine, Massenavette Bruno, Pouyau Robin, Javouhey Etienne
Réanimation pédiatrique, Hôpital Femme Mère Enfant, Hospices Civils de Lyon, 69500, Bron, France.
UMR T_9405, UMRESTTE, Ifsttar, Université Claude Bernard Lyon1, Univ Lyon, 69373, Lyon, France.
Ann Intensive Care. 2017 Dec;7(1):55. doi: 10.1186/s13613-017-0278-1. Epub 2017 May 22.
Asthma is the most common obstructive airway disease in children and adults. Nasal high flow (NHF) is a recent device that is now used as a primary support for respiratory distress. Several studies have reported use of NHF as a respiratory support in status asthmaticus; however, there are no data to recommend such practice. We therefore conducted this preliminary study to evaluate NHF therapy for children with status asthmaticus admitted to our PICU in order to prepare a multicentre randomized controlled study.
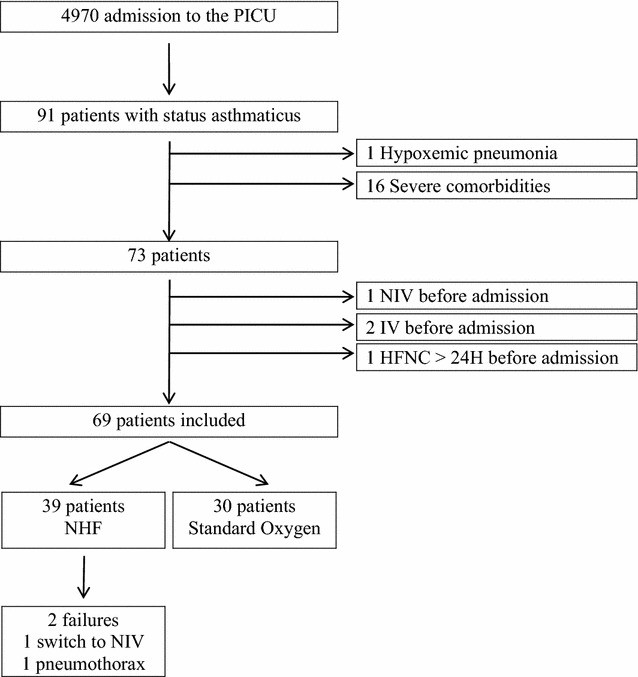
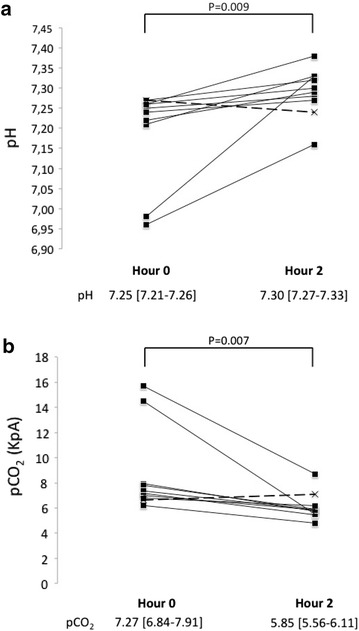
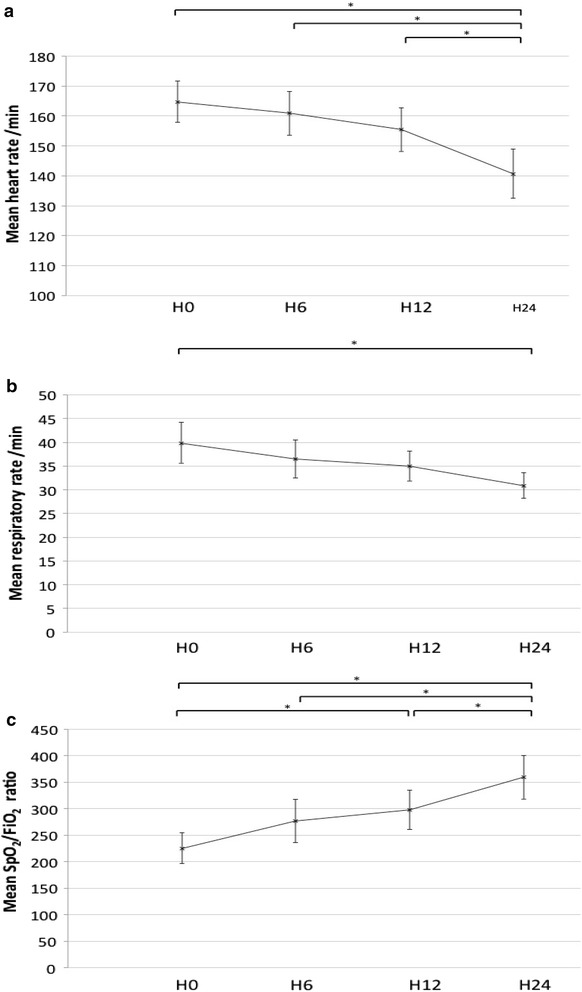
Between November 2009 and January 2014, 73 patients with status asthmaticus were admitted to the PICU, of whom 39 (53%) were treated with NHF and among these 10 (26%) presented severe acidosis at admission (pH < 7.30). Thirty-four less severe children (41%) were treated with standard oxygen. For one child (2.6%) NHF failed and was then switched to non-invasive ventilation. NHF was discontinued in another patient because of the occurrence of pneumothorax after 31 h with NHF; the patient was then switched to standard oxygen therapy. Mean ± SD heart rate (165 ± 21 vs. 141 ± 25/min, p < 0.01) and respiratory rate (40 ± 13 vs. 31 ± 8/min, p < 0.01) decreased significantly, and blood gas improved in the first 24 h. In the subgroup of patients with acidosis, median [IQR] pH increased significantly between hour 0 and 2 (7.25 [7.21-7.26] vs. 7.30 [7.27-7.33], p = 0.009) and median [IQR] pCO decreased significantly (7.27 kPa [6.84-7.91 vs. 5.85 kPa [5.56-6.11], p = 0.007). No patient was intubated.
This retrospective study showed the feasibility and safety of NHF in children with severe asthma. Blood gas and clinical parameters were significantly improved during the first 24 h. NHF failed in only two patients, and none required invasive ventilation.
哮喘是儿童和成人中最常见的阻塞性气道疾病。鼻高流量(NHF)是一种最近开始使用的设备,现被用作呼吸窘迫的主要支持手段。多项研究报道了在哮喘持续状态中使用NHF作为呼吸支持;然而,尚无数据支持这种做法。因此,我们开展了这项初步研究,以评估在我们儿科重症监护病房(PICU)住院的哮喘持续状态儿童使用NHF治疗的效果,以便准备一项多中心随机对照研究。
2009年11月至2014年1月期间,73例哮喘持续状态患者入住PICU,其中39例(53%)接受了NHF治疗,这39例中有10例(26%)入院时出现严重酸中毒(pH < 7.30)。34例病情较轻的儿童(41%)接受了标准吸氧治疗。1例儿童(2.6%)NHF治疗失败,随后改用无创通气。另1例患者在使用NHF 31小时后因发生气胸而停用NHF;该患者随后改用标准吸氧治疗。平均±标准差心率(165±21对141±25次/分钟,p < 0.01)和呼吸频率(40±13对31±8次/分钟,p < 0.01)在最初24小时内显著下降,血气指标得到改善。在酸中毒患者亚组中,0小时和2小时之间pH中位数[四分位间距]显著升高(7.25 [7.21 - 7.26]对7.30 [7.27 - 7.33],p = 0.009),pCO中位数[四分位间距]显著下降(7.27 kPa [6.84 - 7.91]对5.85 kPa [5.56 - 6.11],p = 0.007)。无患者接受气管插管。
这项回顾性研究表明NHF用于重度哮喘儿童具有可行性和安全性。在最初24小时内血气指标和临床参数显著改善。仅2例患者NHF治疗失败,且无人需要有创通气。