O'Brien Megan K, Shawen Nicholas, Mummidisetty Chaithanya K, Kaur Saninder, Bo Xiao, Poellabauer Christian, Kording Konrad, Jayaraman Arun
Max Nader Lab for Rehabilitation Technologies and Outcomes Research, Rehabilitation Institute of Chicago, Chicago, IL, United States.
Department of Physical Medicine and Rehabilitation, Northwestern University, Chicago, IL, United States.
J Med Internet Res. 2017 May 25;19(5):e184. doi: 10.2196/jmir.7385.
Smartphones contain sensors that measure movement-related data, making them promising tools for monitoring physical activity after a stroke. Activity recognition (AR) systems are typically trained on movement data from healthy individuals collected in a laboratory setting. However, movement patterns change after a stroke (eg, gait impairment), and activities may be performed differently at home than in a lab. Thus, it is important to validate AR for gait-impaired stroke patients in a home setting for accurate clinical predictions.
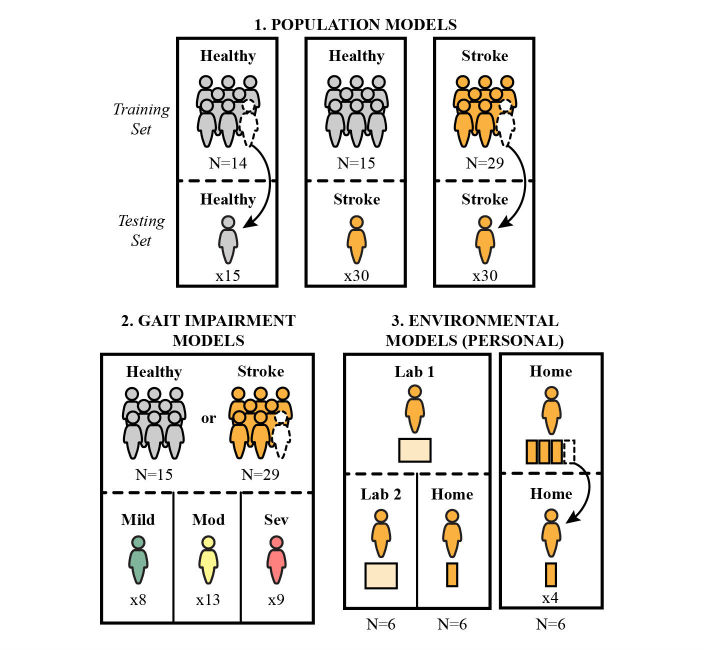
In this study, we sought to evaluate AR performance in a home setting for individuals who had suffered a stroke, by using different sets of training activities. Specifically, we compared AR performance for persons with stroke while varying the origin of training data, based on either population (healthy persons or persons with stoke) or environment (laboratory or home setting).
Thirty individuals with stroke and fifteen healthy subjects performed a series of mobility-related activities, either in a laboratory or at home, while wearing a smartphone. A custom-built app collected signals from the phone's accelerometer, gyroscope, and barometer sensors, and subjects self-labeled the mobility activities. We trained a random forest AR model using either healthy or stroke activity data. Primary measures of AR performance were (1) the mean recall of activities and (2) the misclassification of stationary and ambulatory activities.
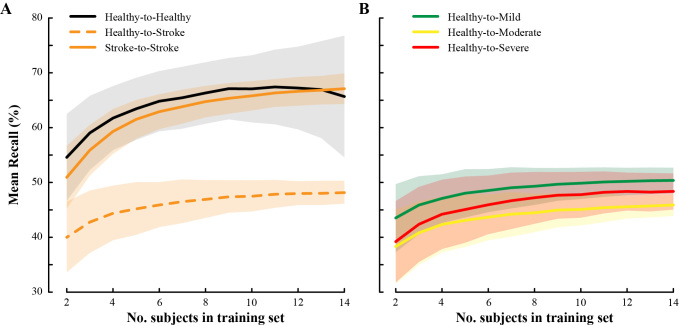
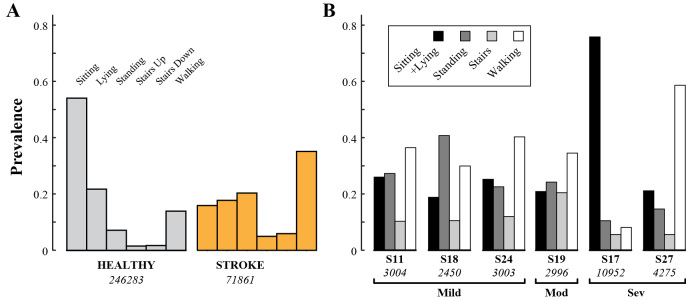
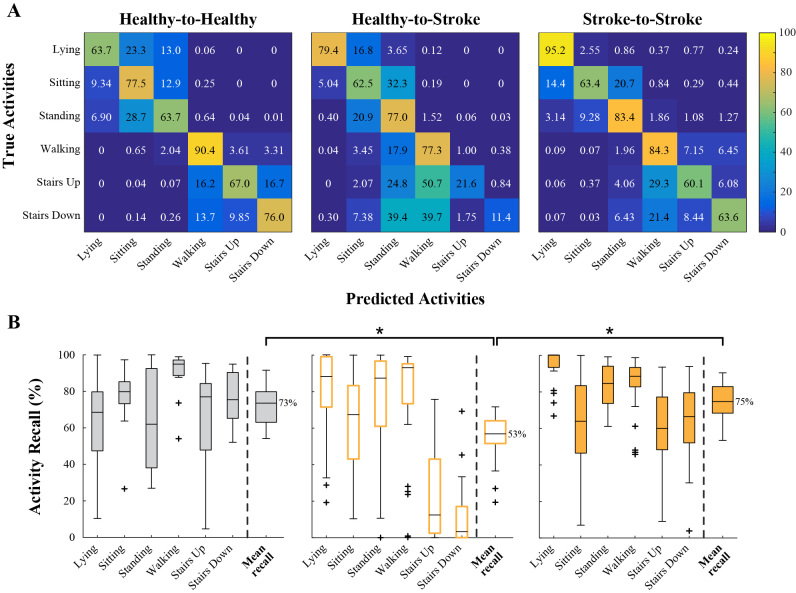
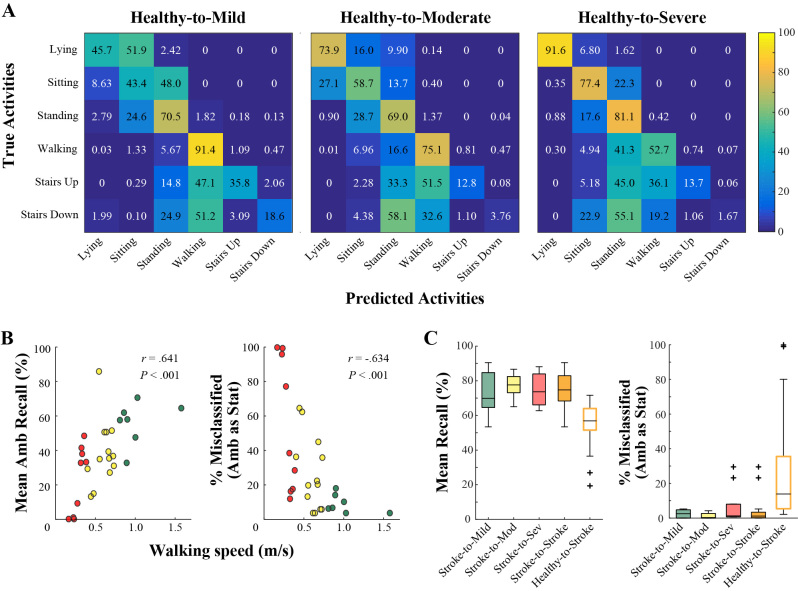
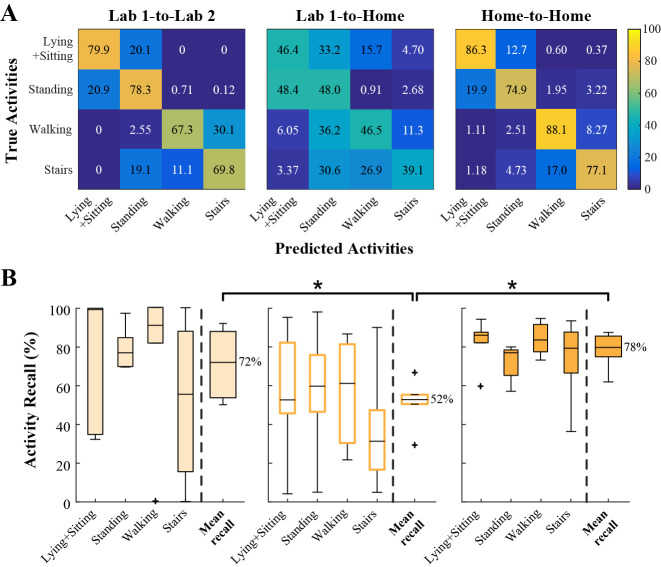
A classifier trained on stroke activity data performed better than one trained on healthy activity data, improving average recall from 53% to 75%. The healthy-trained classifier performance declined with gait impairment severity, more often misclassifying ambulatory activities as stationary ones. The classifier trained on in-lab activities had a lower average recall for at-home activities (56%) than for in-lab activities collected on a different day (77%).
Stroke-based training data is needed for high quality AR among gait-impaired individuals with stroke. Additionally, AR systems for home and community monitoring would likely benefit from including at-home activities in the training data.
智能手机包含可测量与运动相关数据的传感器,使其成为中风后监测身体活动的有前景的工具。活动识别(AR)系统通常在实验室环境中收集的健康个体的运动数据上进行训练。然而,中风后运动模式会发生变化(例如步态障碍),并且活动在家庭中的执行方式可能与在实验室中不同。因此,在家庭环境中验证针对步态受损中风患者的AR以进行准确的临床预测很重要。
在本研究中,我们试图通过使用不同的训练活动集来评估家庭环境中中风患者的AR性能。具体而言,我们基于人群(健康人或中风患者)或环境(实验室或家庭环境)改变训练数据的来源,比较中风患者的AR性能。
30名中风患者和15名健康受试者在佩戴智能手机的情况下,在实验室或家中进行了一系列与移动性相关的活动。一个定制应用程序收集来自手机加速度计、陀螺仪和气压计传感器的信号,受试者对移动性活动进行自我标记。我们使用健康或中风活动数据训练了一个随机森林AR模型。AR性能的主要指标是(1)活动的平均召回率和(2)静止和动态活动的错误分类。
在中风活动数据上训练的分类器比在健康活动数据上训练的分类器表现更好,将平均召回率从53%提高到了75%。健康训练的分类器性能随着步态障碍严重程度的增加而下降,更常将动态活动错误分类为静止活动。在实验室活动上训练的分类器对家庭活动的平均召回率(56%)低于在不同日期收集的实验室活动的平均召回率(77%)。
对于步态受损的中风患者,高质量的AR需要基于中风的训练数据。此外,用于家庭和社区监测的AR系统可能会从将家庭活动纳入训练数据中受益。