Bowman Kirsty, Atkins Janice L, Delgado João, Kos Katarina, Kuchel George A, Ble Alessandro, Ferrucci Luigi, Melzer David
Epidemiology and Public Health Group and.
Diabetes and Obesity Research Group, Institute of Biomedical and Clinical Sciences, University of Exeter Medical School, Exeter, United Kingdom.
Am J Clin Nutr. 2017 Jul;106(1):130-135. doi: 10.3945/ajcn.116.147157. Epub 2017 May 31.
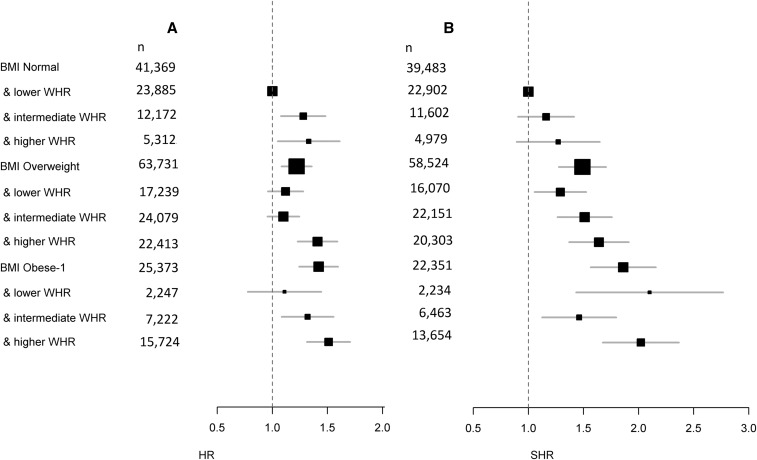
For older groups, being overweight [body mass index (BMI; in kg/m): 25 to <30] is reportedly associated with a lower or similar risk of mortality than being normal weight (BMI: 18.5 to <25). However, this "risk paradox" is partly explained by smoking and disease-associated weight loss. This paradox may also arise from BMI failing to measure fat redistribution to a centralized position in later life. This study aimed to estimate associations between combined measurements of BMI and waist-to-hip ratio (WHR) with mortality and incident coronary artery disease (CAD). This study followed 130,473 UK Biobank participants aged 60-69 y (baseline 2006-2010) for ≤8.3 y ( = 2974 deaths). Current smokers and individuals with recent or disease-associated (e.g., from dementia, heart failure, or cancer) weight loss were excluded, yielding a "healthier agers" group. Survival models were adjusted for age, sex, alcohol intake, smoking history, and educational attainment. Population and sex-specific lower and higher WHR tertiles were <0.91 and ≥0.96 for men and <0.79 and ≥0.85 for women, respectively. Ignoring WHR, the risk of mortality for overweight subjects was similar to that for normal-weight subjects (HR: 1.09; 95% CI: 0.99, 1.19; = 0.066). However, among normal-weight subjects, mortality increased for those with a higher WHR (HR: 1.33; 95% CI: 1.08, 1.65) compared with a lower WHR. Being overweight with a higher WHR was associated with substantial excess mortality (HR: 1.41; 95% CI: 1.25, 1.61) and greatly increased CAD incidence (sub-HR: 1.64; 95% CI: 1.39, 1.93) compared with being normal weight with a lower WHR. There was no interaction between physical activity and BMI plus WHR groups with respect to mortality. For healthier agers (i.e., nonsmokers without disease-associated weight loss), having central adiposity and a BMI corresponding to normal weight or overweight is associated with substantial excess mortality. The claimed BMI-defined overweight risk paradox may result in part from failing to account for central adiposity, rather than reflecting a protective physiologic effect of higher body-fat content in later life.
据报道,对于老年人群体,超重(体重指数(BMI;单位:kg/m²):25至<30)与正常体重(BMI:18.5至<25)相比,死亡风险更低或相似。然而,这种“风险悖论”部分可由吸烟和疾病相关的体重减轻来解释。这种悖论也可能源于BMI未能衡量晚年脂肪向身体中心部位的重新分布。本研究旨在评估BMI与腰臀比(WHR)的联合测量值与死亡率及冠心病(CAD)发病率之间的关联。本研究对130473名年龄在60 - 69岁(基线为2006 - 2010年)的英国生物银行参与者进行了长达≤8.3年的随访(共2974人死亡)。排除当前吸烟者以及近期有体重减轻或因疾病(如痴呆、心力衰竭或癌症)导致体重减轻的个体,从而形成一个“更健康的老年人”群体。生存模型根据年龄、性别、酒精摄入量、吸烟史和教育程度进行了调整。按人群和性别划分,较低和较高WHR三分位数男性分别为<0.91和≥0.96,女性分别为<0.79和≥0.85。忽略WHR,超重受试者的死亡风险与正常体重受试者相似(风险比:1.09;95%置信区间:0.99,1.19;P = 0.066)。然而,在正常体重受试者中,与较低WHR者相比,较高WHR者的死亡率增加(风险比:1.33;95%置信区间:1.08,1.65)。与较低WHR的正常体重者相比,较高WHR的超重者与显著更高的死亡率(风险比:1.41;95%置信区间:1.25,1.61)及大幅增加的CAD发病率相关(亚风险比:1.64;95%置信区间:1.39,1.93)。在死亡率方面,身体活动与BMI加WHR分组之间没有相互作用。对于更健康的老年人(即无疾病相关体重减轻的非吸烟者),中心性肥胖且BMI对应正常体重或超重与显著更高的死亡率相关。所谓的由BMI定义的超重风险悖论可能部分是由于未考虑中心性肥胖,而非反映晚年较高体脂含量的保护生理效应。