Jung Jang Han, Lee Hyun Jik, Lee Hee Seung, Jo Jung Hyun, Cho In Rae, Chung Moon Jae, Park Jeong Youp, Park Seung Woo, Song Si Young, Bang Seungmin
Jang Han Jung, Division of Gastroenterology, Department of Internal Medicine, Hallym University Dongtan Sacred Heart Hospital, 7, Keunjaebong-gil, Hwaseong-si, Gyeonggi-do 18450, South Korea.
World J Gastroenterol. 2017 May 14;23(18):3301-3308. doi: 10.3748/wjg.v23.i18.3301.
To clarify the role of neoadjuvant concurrent chemoradiotherapy (NACCRT) followed by surgical resection for localized or locally advanced perihilar cholangiocarcinoma (CCA).
We retrospectively reviewed 57 patients who underwent surgical resection with or without NACCRT for perihilar CCA; 12 patients received NACCRT and 45 patients did not received NACCRT. Patients with locally advanced perihilar CCA requiring NACCRT were defined as follows: (1) a mass involving unilateral branches of the portal vein or hepatic artery with insufficient volume of the anticipated remnant lobe; or (2) an infiltrating mass in the main portal vein that was too long for reconstruction, identified at preoperative staging.
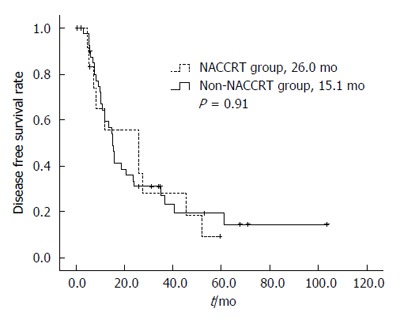
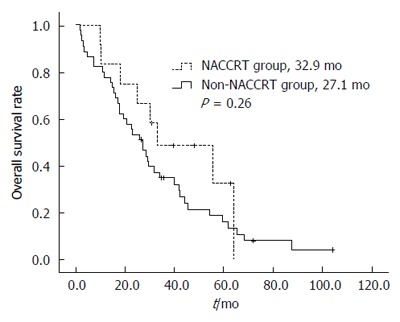
The median disease-free survival (DFS) durations of the neoadjuvant and non-neoadjuvant CCRT groups were 26.0 and 15.1 mo, respectively ( = 0.91). The median overall survival (OS) durations of the neoadjuvant and non-neoadjuvant CCRT groups were 32.9 and 27.1 mo, respectively ( = 0.26). The NACCRT group showed a downstaging tendency compared to the non-NACCRT group as compared with the tumor stage confirmed by histological examination after surgery and the tumor stage confirmed by imaging test at the time of diagnosis ( = 0.01).
NACCRT does not prolong DFS and OS in localized or locally advanced perihilar CCA. However, NACCRT may allow tumor downstaging and improve tumor resectability.
明确新辅助同步放化疗(NACCRT)后行手术切除在局限性或局部进展期肝门部胆管癌(CCA)中的作用。
我们回顾性分析了57例行肝门部CCA手术切除的患者,其中12例接受了NACCRT,45例未接受NACCRT。需要NACCRT的局部进展期肝门部CCA患者定义如下:(1)肿块累及门静脉或肝动脉的单侧分支,预期剩余肝叶体积不足;或(2)术前分期发现主门静脉内浸润性肿块过长无法重建。
新辅助和非新辅助CCRT组的无病生存期(DFS)中位数分别为26.0个月和15.1个月(=0.91)。新辅助和非新辅助CCRT组的总生存期(OS)中位数分别为32.9个月和27.1个月(=0.26)。与非NACCRT组相比,NACCRT组在术后组织学检查证实的肿瘤分期和诊断时影像学检查证实的肿瘤分期方面显示出降期趋势(=0.01)。
NACCRT不能延长局限性或局部进展期肝门部CCA的DFS和OS。然而,NACCRT可能使肿瘤降期并提高肿瘤切除率。