van Kessel Emma, Baumfalk Anniek E, van Zandvoort Martine J E, Robe Pierre A, Snijders Tom J
Department of Neurology & Neurosurgery, University Medical Center Utrecht/Brain Center Rudolf Magnus, G03.232, PO Box 85500, 3508 XC, Utrecht, The Netherlands.
Helmhotz Institute, Utrecht University, Room 1715, Heidelberglaan 1, 3584 CS, Utrecht, The Netherlands.
J Neurooncol. 2017 Aug;134(1):9-18. doi: 10.1007/s11060-017-2503-z. Epub 2017 May 31.
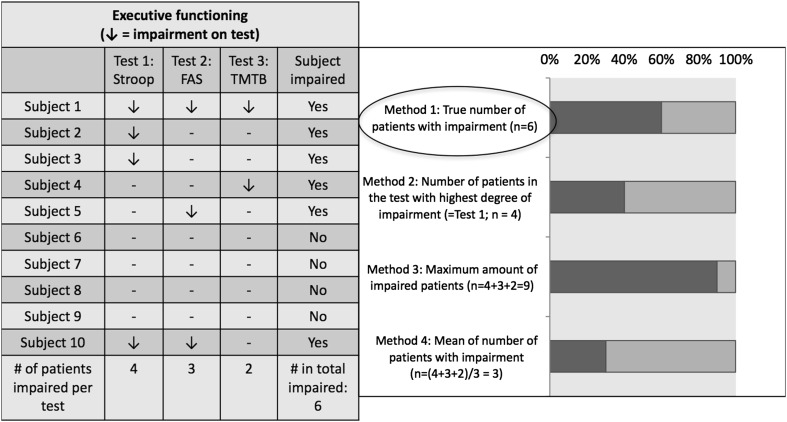
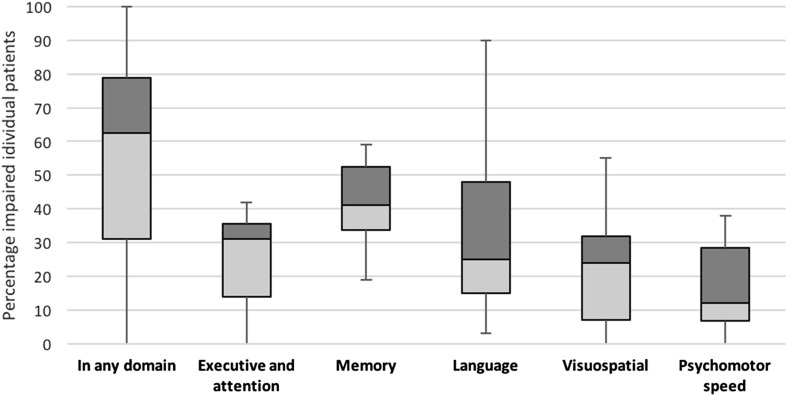
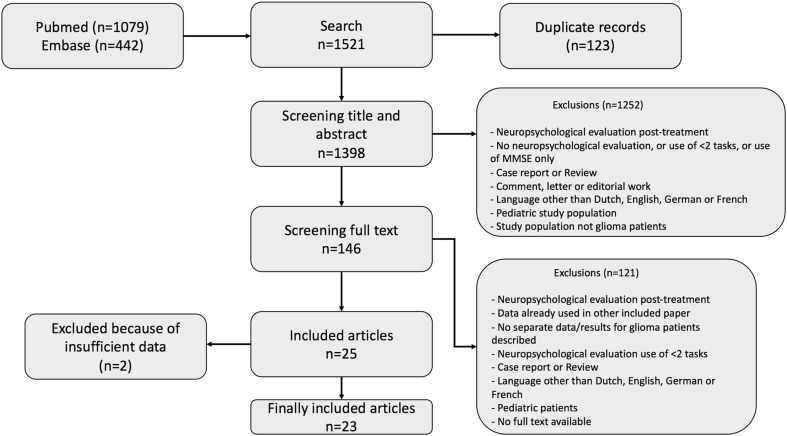
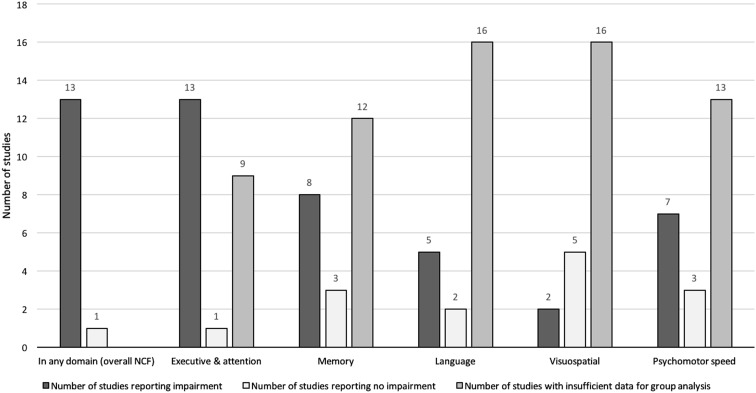
Deficits in neurocognitive functioning (NCF) frequently occur in glioma patients. Both treatment and the tumor itself contribute to these deficits. Data about the role of the tumor are scarce, because NCF has mostly been studied postoperatively. We aimed to summarize data on pre-treatment NCF in glioma patients and to determine the overall and domain-specific prevalence of neurocognitive dysfunction. We searched PubMed and Embase according to PRISMA-P protocol for studies that evaluated pre-treatment NCF in glioma patients (1995-November 2016) and extracted information about NCF. We performed analysis of data for two main outcome measures; mean cognitive functioning of the study sample (at group level) and the percentage of impaired patients (at individual level). We included 23 studies. Most studies were small observational prospective cohort studies. In 11 (47.5%) studies, patient selection was based on tumor location. NCF was analyzed at the group level in 14 studies, of which 13 (92.9%) found decreased NCF at group level, compared to normative data or matched controls. The proportion of individuals with decreased NCF was reported in 15 studies. NCF was impaired (in any domain) in 62.6% of the individuals (median; interquartile range 31.0-79.0). Cognitive impairments were more common in patients with high-grade glioma than with low-grade glioma (OR 2.50; 95% CI 1.71-3.66). Cognitive impairment occurs in the majority of treatment-naive glioma patients, suggesting that neurocognitive dysfunction is related to the tumor. However, the literature about pre-treatment NCF in glioma patients is characterized by small-scale studies and strong heterogeneity in patient selection, resulting in high risk of bias.
神经认知功能(NCF)缺陷在胶质瘤患者中经常出现。治疗和肿瘤本身都会导致这些缺陷。关于肿瘤作用的数据很少,因为NCF大多是在术后进行研究的。我们旨在总结胶质瘤患者治疗前NCF的数据,并确定神经认知功能障碍的总体患病率和特定领域患病率。我们根据PRISMA-P协议在PubMed和Embase上搜索评估胶质瘤患者治疗前NCF的研究(1995年至2016年11月),并提取有关NCF的信息。我们对两项主要结局指标的数据进行了分析;研究样本的平均认知功能(组水平)和受损患者的百分比(个体水平)。我们纳入了23项研究。大多数研究是小型观察性前瞻性队列研究。在11项(47.5%)研究中,患者选择基于肿瘤位置。14项研究在组水平分析了NCF,其中13项(92.9%)发现与标准数据或匹配对照相比,组水平的NCF降低。15项研究报告了NCF降低的个体比例。62.6%的个体(中位数;四分位间距31.0 - 79.0)存在NCF受损(任何领域)。高级别胶质瘤患者比低级别胶质瘤患者更常见认知障碍(OR 2.50;95% CI 1.71 - 3.66)。大多数未经治疗的胶质瘤患者存在认知障碍,这表明神经认知功能障碍与肿瘤有关。然而,关于胶质瘤患者治疗前NCF的文献具有研究规模小和患者选择存在强烈异质性的特点,导致偏倚风险高。