Vijgen Leen, Thys Kim, Vandebosch An, Van Remoortere Pieter, Verloes René, De Meyer Sandra
Janssen Research & Development, Janssen Pharmaceutica NV, Turnhoutseweg 30, 2340, Beerse, Belgium.
Virol J. 2017 May 31;14(1):101. doi: 10.1186/s12985-017-0760-2.
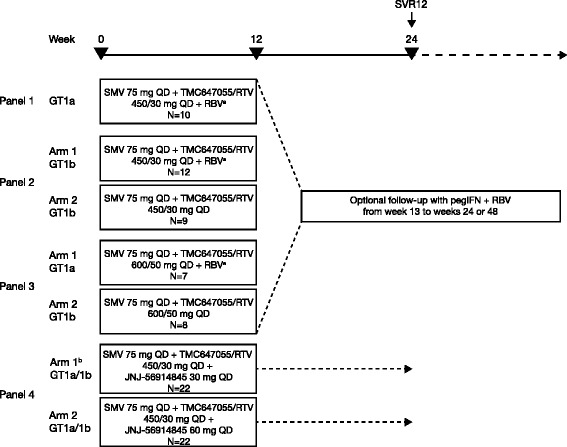
In study TMC647055HPC2001, a 3-direct-acting-antiviral (DAA) regimen combining NS3/4A protease inhibitor simeprevir (SMV), non-nucleoside NS5B inhibitor TMC647055/ritonavir (RTV) and NS5A inhibitor JNJ-56914845 resulted in high sustained virologic response 12 weeks after actual end of treatment (SVR12) in chronic hepatitis C virus (HCV) genotype 1-infected patients. SVR12 rates were generally lower in the 2-DAA regimen SMV + TMC647055/RTV with or without ribavirin. The objective of this study was to identify and characterise pre-existing and emerging resistance-associated variants (RAVs) in patients enrolled in study TMC647055HPC2001.
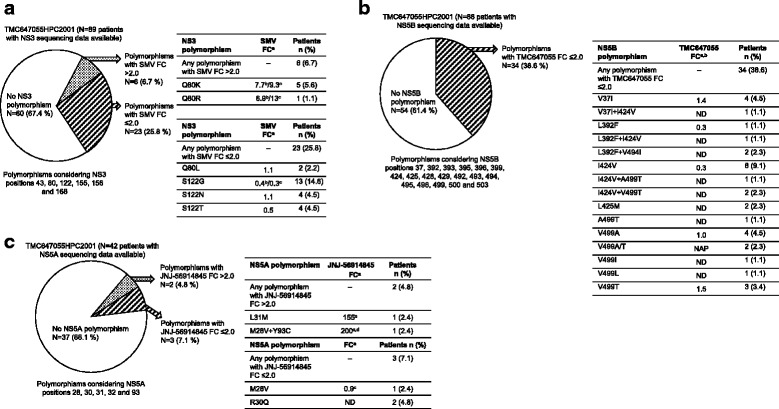
HCV population sequencing analyses were performed on baseline isolates from all patients (n = 90) and post-baseline isolates from patients with virologic failure (n = 22). In addition, deep sequencing and phenotypic analyses were performed on selected baseline and post-baseline isolates.
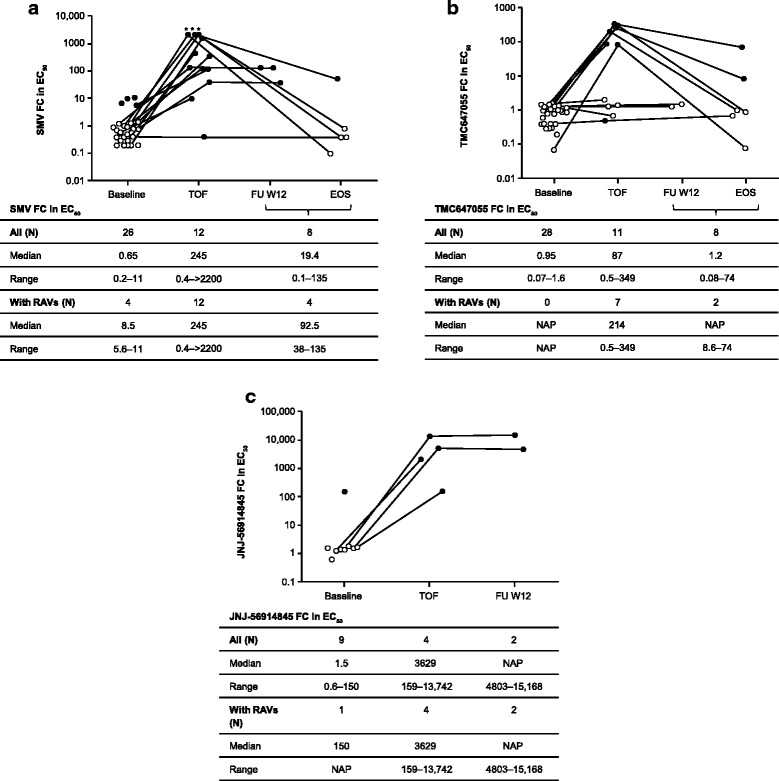
The majority of patients with virologic failure had emerging RAVs to all study drugs at the time of failure: in all 22 patients SMV RAVs emerged at NS3 positions 80, 155, 156 and/or 168, consistent with the known SMV resistance profile. Emerging TMC647055 RAVs at NS5B position 495 were detected in the majority of patients (16/22), and all 5 patients who failed the 3-DAA regimen had emerging JNJ-56914845 RAVs at NS5A positions 30 and/or 31. While at the end of study emerging SMV and TMC647055 RAVs were no longer observed by population sequencing in 40% (8/20) and 62.5% (10/16) of patients with follow-up data available, respectively, emerging JNJ-56914845 RAVs were still detected in all (5/5) patients.
Virologic failure in the 2- and 3-DAA combinations was, in the majority of patients, associated with the emergence of RAVs to all study drugs. While emerging SMV and TMC647055 RAVs became undetectable during follow-up, JNJ-56914845 RAVs in NS5A were still observed at end of study.
NCT01724086 (date of registration: September 26, 2012).
在研究TMC647055HPC2001中,一种由NS3/4A蛋白酶抑制剂西美瑞韦(SMV)、非核苷类NS5B抑制剂TMC647055/利托那韦(RTV)和NS5A抑制剂JNJ - 56914845组成的三联直接抗病毒(DAA)方案,使慢性丙型肝炎病毒(HCV)1型感染患者在实际治疗结束后12周实现了高持续病毒学应答(SVR12)。在含或不含利巴韦林的二联DAA方案SMV + TMC647055/RTV中,SVR12率通常较低。本研究的目的是鉴定和表征参与研究TMC647055HPC2001的患者中预先存在的和新出现的耐药相关变异(RAV)。
对所有患者(n = 90)的基线分离株以及病毒学失败患者(n = 22)的基线后分离株进行HCV群体测序分析。此外,对选定的基线和基线后分离株进行深度测序和表型分析。
大多数病毒学失败患者在失败时出现了对所有研究药物的新RAV:在所有22例患者中,SMV的RAV出现在NS3的80、155、156和/或168位,与已知的SMV耐药谱一致。大多数患者(16/22)检测到NS5B第495位出现新的TMC647055 RAV,在三联DAA方案中失败的所有5例患者在NS5A的30和/或31位出现了新的JNJ - 56914845 RAV。虽然在研究结束时,在有随访数据的患者中,分别有40%(8/20)和62.5%(10/16)通过群体测序不再观察到新出现的SMV和TMC647055 RAV,但在所有(5/5)患者中仍检测到新出现的JNJ - 56914845 RAV。
在大多数患者中,二联和三联DAA方案中的病毒学失败与对所有研究药物的RAV出现有关。虽然在随访期间新出现的SMV和TMC647055 RAV变得不可检测,但在研究结束时仍观察到NS5A中的JNJ - 56914845 RAV。
NCT01724086(注册日期:2012年9月26日)。