Long Qian, Allanson Emma R, Pontre Jennifer, Tunçalp Özge, Hofmeyr George Justus, Gülmezoglu Ahmet Metin
Department of Reproductive Health and Research, UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP), World Health Organization, Geneva, Switzerland.
Faculty of Medicine, Dentistry and Health Sciences, School of Women's and Infants' Health, University of Western Australia, Crawley, Australia.
BMJ Glob Health. 2016 Sep 2;1(2):e000096. doi: 10.1136/bmjgh-2016-000096. eCollection 2016.
To ensure timely access to comprehensive emergency obstetric care in low- and middle-income countries, a number of interventions have been employed. This systematic review assesses the effects of onsite midwife-led birth units (OMBUs) embedded within hospitals which provide comprehensive emergency obstetric and newborn care.
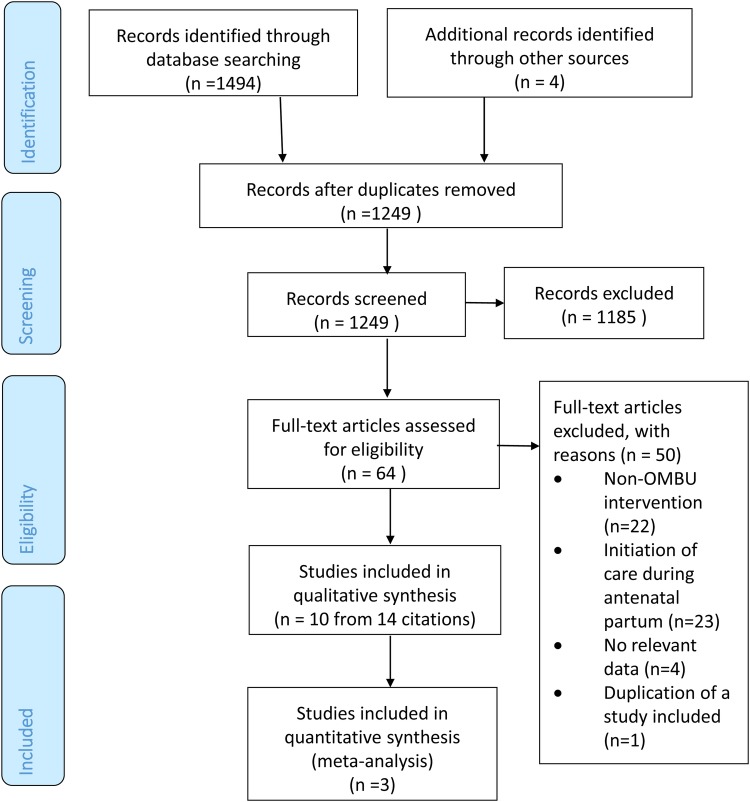
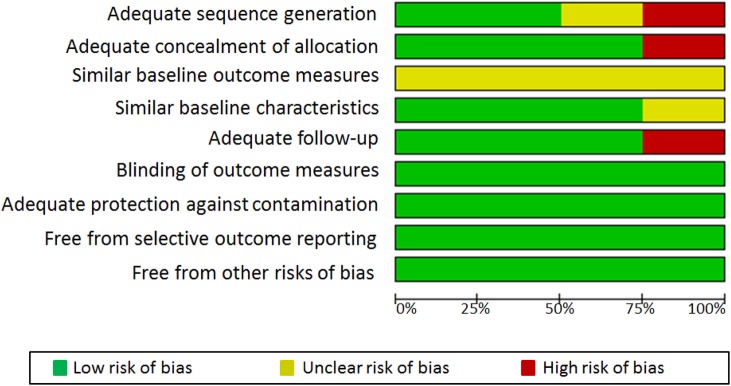
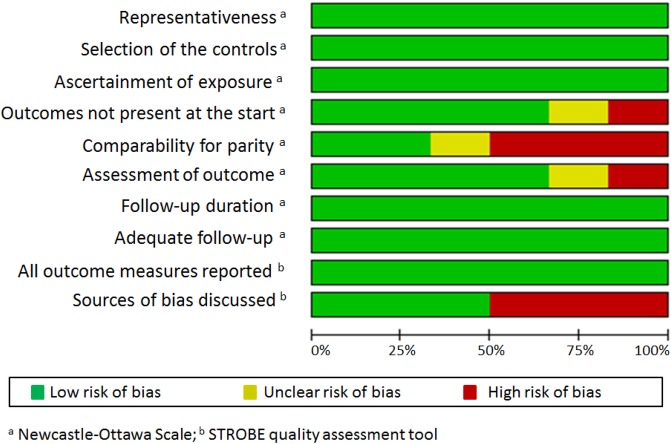
Both interventional and observational studies that compared OMBUs with standard medical-led obstetric care were eligible for inclusion. Cochrane Central Register of Controlled Trials, PubMed/Medline, EMBASE, CINAHL, Science Citation and Social Sciences Citation Index, Global Health Library and one Chinese database were searched. Meta-analysis was conducted to synthesise data from randomised controlled trials (RCTs). Findings of observational studies were summarised by forest plots with brief narratives.
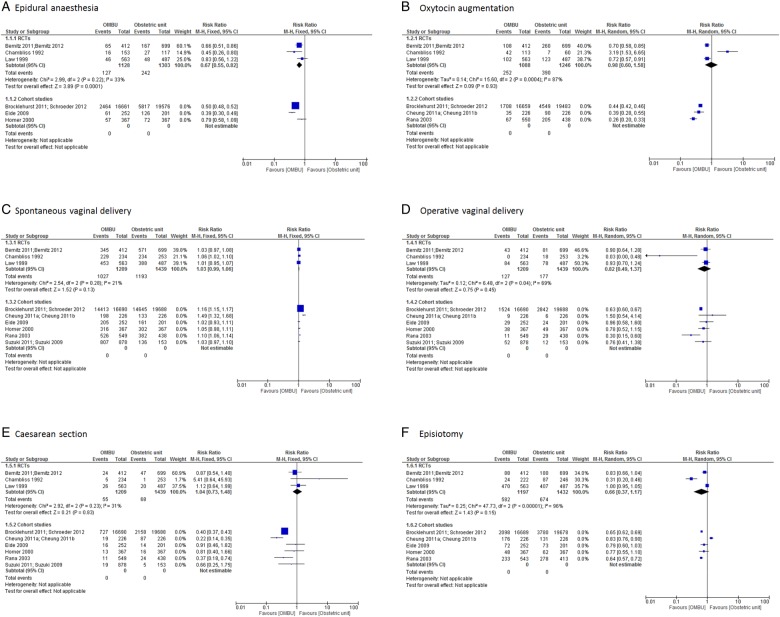
Three RCTs, one controlled before-and-after study and six cohort studies were included. There were no or very few maternal and perinatal deaths in either OMBUs or standard obstetric units, with no significant differences between the two. Women giving birth in OMBUs were less likely to use epidural analgesia (risk ratio (RR) 0.67, 95% CI 0.55 to 0.82; three trials, n=2431). The UK national cohort study and two other cohorts in China and Nepal found less oxytocin augmentation, more spontaneous vaginal deliveries, fewer caesarean sections and fewer episiotomies performed in OMBUs than in standard obstetric units. These differences were not statistically significant in RCTs and the remaining cohorts. One study investigated satisfaction with midwife-led birth care among women and midwives, with positive findings in both groups favouring OMBUs. In addition, two studies found that the total cost of birth was lower in OMBUs than in standard obstetric units.
OMBUs could be an alternative model for providing safe and cost-effective childbirth care, which may be particularly important in low- and middle-income countries to meet the growing demand for facility-based birth for low-risk women and improve efficiency of health systems.
为确保低收入和中等收入国家能够及时获得全面的紧急产科护理,已采取了一系列干预措施。本系统评价评估了医院内由助产士主导的现场分娩单元(OMBU)对提供全面的紧急产科和新生儿护理的效果。
比较OMBU与标准医疗主导的产科护理的干预性研究和观察性研究均符合纳入标准。检索了Cochrane对照试验中心注册库、PubMed/Medline、EMBASE、CINAHL、科学引文索引和社会科学引文索引、全球健康图书馆以及一个中文数据库。对随机对照试验(RCT)的数据进行荟萃分析。观察性研究的结果通过森林图和简短叙述进行总结。
纳入了三项RCT、一项前后对照研究和六项队列研究。OMBU或标准产科单元的孕产妇和围产儿死亡均极少或没有,两者之间无显著差异。在OMBU分娩的妇女使用硬膜外镇痛的可能性较小(风险比(RR)0.67,95%置信区间0.55至0.82;三项试验,n = 2431)。英国全国队列研究以及中国和尼泊尔的另外两项队列研究发现,与标准产科单元相比,OMBU中催产素使用增加较少、自然阴道分娩较多、剖宫产较少且会阴切开术较少。这些差异在RCT和其余队列中无统计学意义。一项研究调查了妇女和助产士对助产士主导的分娩护理的满意度,两组均对OMBU有积极评价。此外,两项研究发现OMBU的分娩总成本低于标准产科单元。
OMBU可能是提供安全且具成本效益的分娩护理的一种替代模式,这在低收入和中等收入国家可能尤为重要,以满足低风险妇女对机构分娩日益增长的需求并提高卫生系统的效率。