McBain Ryan K, Jerome Gregory, Warsh Jonathan, Browning Micaela, Mistry Bipin, Faure Peterson Abnis I, Pierre Claire, Fang Anna P, Mugunga Jean Claude, Rhatigan Joseph, Leandre Fernet, Kaplan Robert
Partners in Health, Boston, Massachusetts, USA.
Zanmi Lasante, Port-au-Prince, Haiti.
BMJ Glob Health. 2016 Nov 11;1(3):e000134. doi: 10.1136/bmjgh-2016-000134. eCollection 2016.
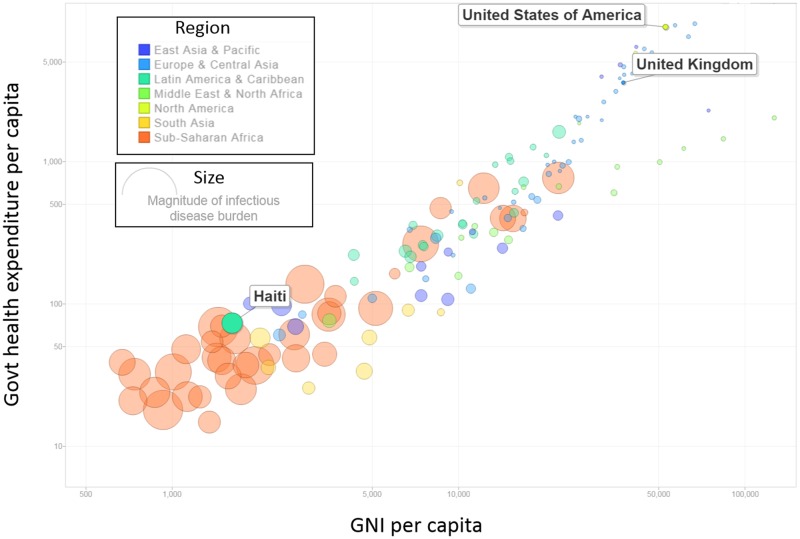
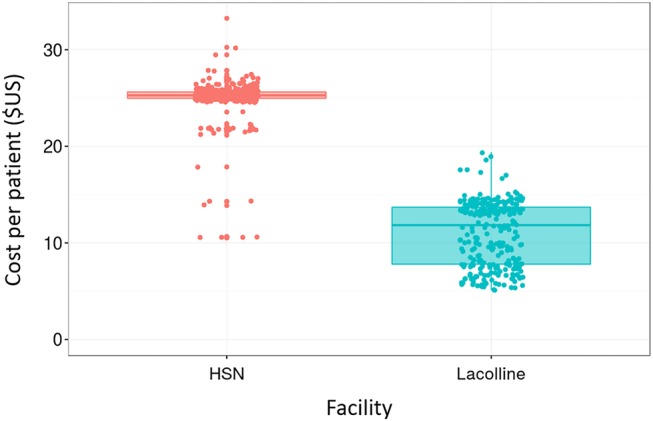
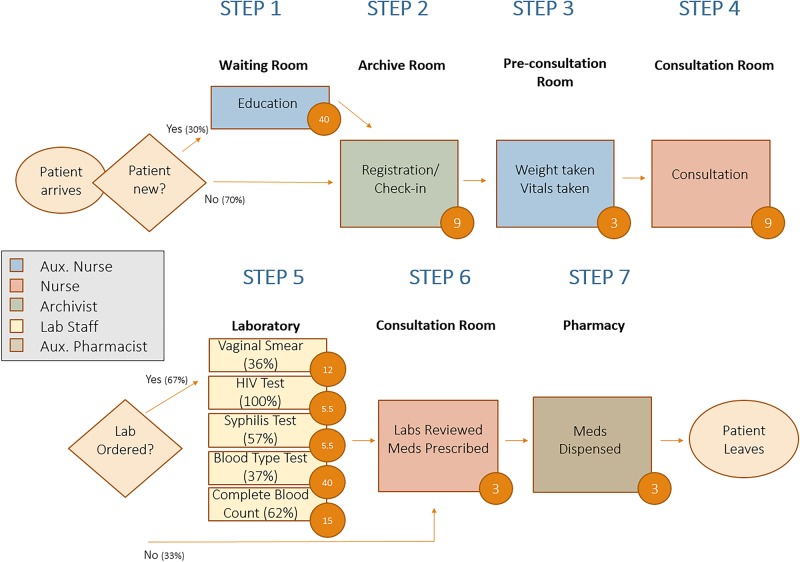
Low-income and middle-income countries account for over 80% of the world's infectious disease burden, but <20% of global expenditures on health. In this context, judicious resource allocation can mean the difference between life and death, not just for individual patients, but entire patient populations. Understanding the cost of healthcare delivery is a prerequisite for allocating health resources, such as staff and medicines, in a way that is effective, efficient, just and fair. Nevertheless, health costs are often poorly understood, undermining effectiveness and efficiency of service delivery. We outline shortcomings, and consequences, of common approaches to estimating the cost of healthcare in low-resource settings, as well as advantages of a newly introduced approach in healthcare known as time-driven activity-based costing (TDABC). TDABC is a patient-centred approach to cost analysis, meaning that it begins by studying the flow of individual patients through the health system, and measuring the human, equipment and facility resources used to treat the patients. The benefits of this approach are numerous: fewer assumptions need to be made, heterogeneity in expenditures can be studied, service delivery can be modelled and streamlined and stronger linkages can be established between resource allocation and health outcomes. TDABC has demonstrated significant benefits for improving health service delivery in high-income countries but has yet to be adopted in resource-limited settings. We provide an illustrative case study of its application throughout a network of hospitals in Haiti, as well as a simplified framework for policymakers to apply this approach in low-resource settings around the world.
低收入和中等收入国家承担着全球80%以上的传染病负担,但在全球卫生支出中所占比例却不到20%。在这种背景下,明智地分配资源可能意味着生与死的差别,这不仅关乎个体患者,还涉及全体患者群体。了解医疗服务的成本是有效、高效、公正且公平地分配卫生资源(如人员和药品)的前提条件。然而,人们往往对卫生成本了解不足,这削弱了服务提供的有效性和效率。我们概述了在资源匮乏环境中估算医疗成本的常见方法的缺点及后果,以及一种新引入的医疗成本核算方法——时间驱动作业成本法(TDABC)的优势。TDABC是一种以患者为中心的成本分析方法,即首先研究个体患者在卫生系统中的就医流程,并衡量治疗患者所使用的人力、设备和设施资源。这种方法的益处众多:需要做出的假设更少,可以研究支出的异质性,可以对服务提供进行建模和简化,并且可以在资源分配与健康结果之间建立更紧密的联系。TDABC已在高收入国家证明了对改善卫生服务提供具有显著益处,但在资源有限的环境中尚未得到采用。我们提供了一个在海地的医院网络中应用TDABC的案例研究示例,以及一个简化框架,供政策制定者在全球资源匮乏环境中应用这种方法。