Division of Surgery and Interventional Science, University College London, UK.
Anaesthesia and Critical Care Research Unit, University Hospital Southampton NHS Foundation Trust, Southampton, UK.
Haematologica. 2017 Sep;102(9):1477-1485. doi: 10.3324/haematol.2017.169680. Epub 2017 Jun 8.
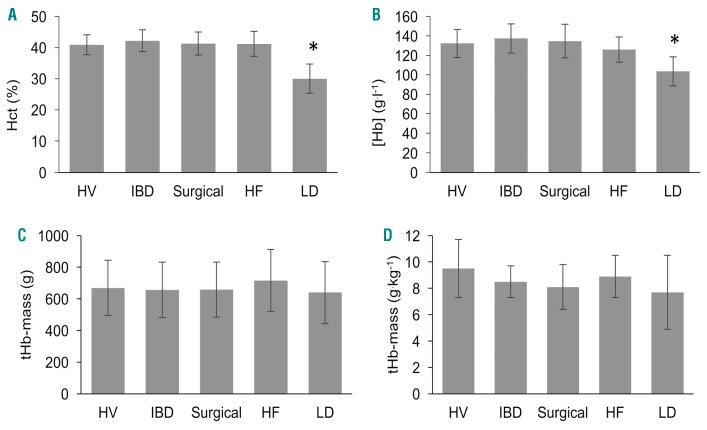
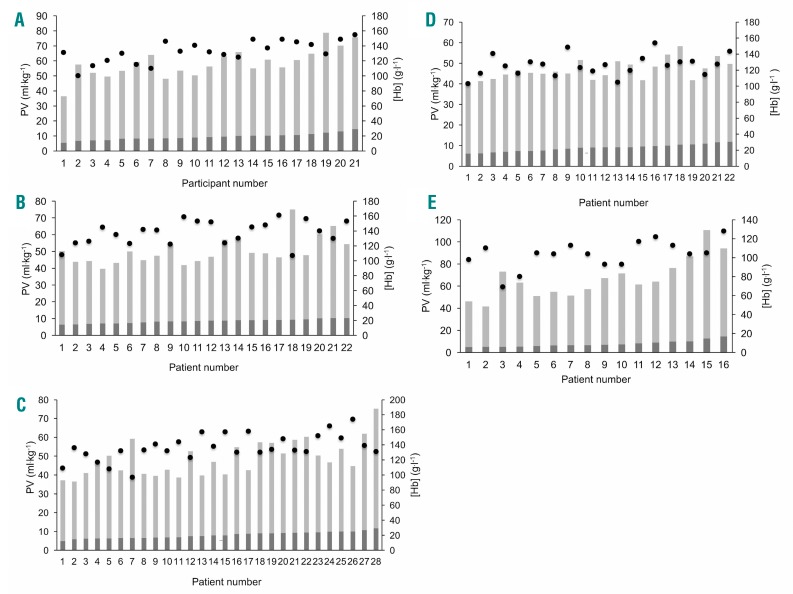
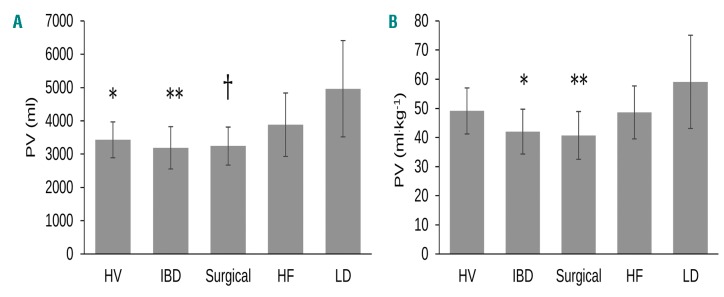
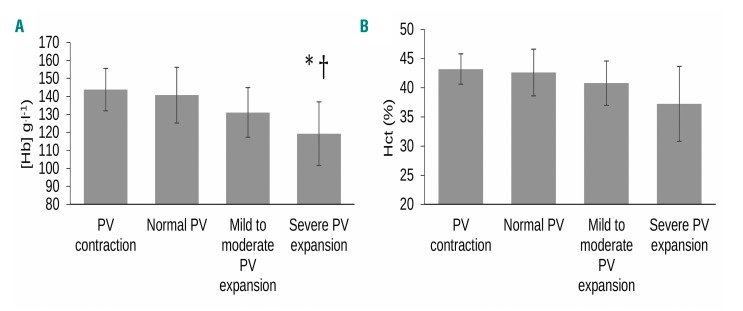
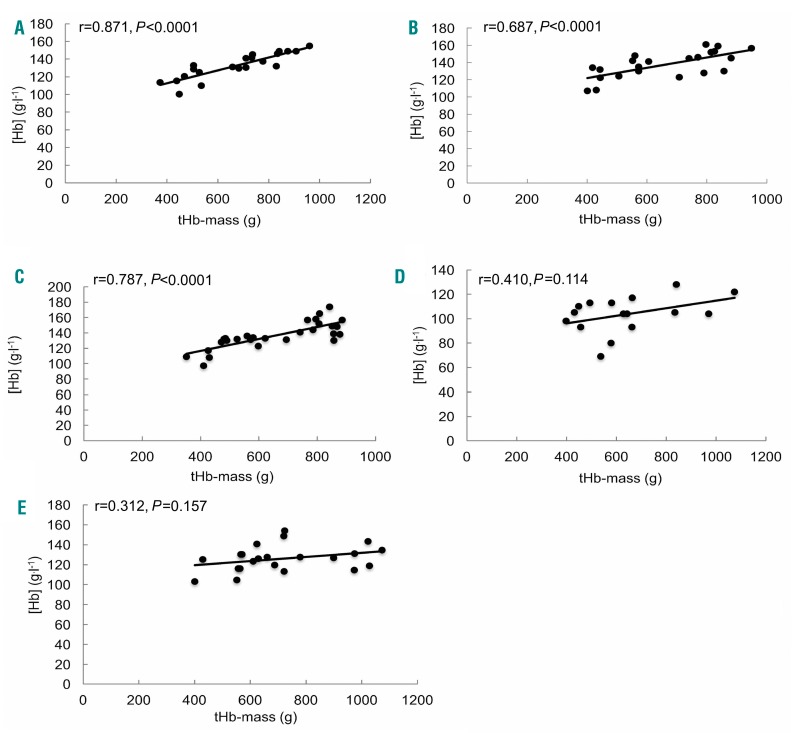
In practice, clinicians generally consider anemia (circulating hemoglobin concentration < 120 g.l in non-pregnant females and < 130 g.l in males) as due to impaired hemoglobin synthesis or increased erythrocyte loss or destruction. Rarely is a rise in plasma volume relative to circulating total hemoglobin mass considered as a cause. But does this matter? We explored this issue in patients, measuring hemoglobin concentration, total hemoglobin mass (optimized carbon monoxide rebreathing method) and thereby calculating plasma volume in healthy volunteers, surgical patients, and those with inflammatory bowel disease, chronic liver disease or heart failure. We studied 109 participants. Hemoglobin mass correlated well with its concentration in the healthy, surgical and inflammatory bowel disease groups (r=0.687-0.871, <0.001). However, they were poorly related in liver disease (r=0.410, =0.11) and heart failure patients (r=0.312, =0.16). Here, hemoglobin mass explained little of the variance in its concentration (adjusted R=0.109 and 0.052; =0.11 and 0.16), whilst plasma volume did (R change 0.724 and 0.805 in heart and liver disease respectively, <0.0001). Exemplar patients with identical (normal or raised) total hemoglobin masses were diagnosed as profoundly anemic (or not) depending on differences in plasma volume that had not been measured or even considered as a cause. The traditional inference that anemia generally reflects hemoglobin deficiency may be misleading, potentially resulting in inappropriate tests and therapeutic interventions to address 'hemoglobin deficiency' not 'plasma volume excess'. Measurement of total hemoglobin mass and plasma volume is now simple, cheap and safe, and its more routine use is advocated.
在实践中,临床医生通常将贫血(非妊娠女性循环血红蛋白浓度<120g/L,男性<130g/L)归因于血红蛋白合成受损或红细胞丢失或破坏增加。很少考虑血浆量相对于循环总血红蛋白质量的增加是一个原因。但这有关系吗?我们在健康志愿者、手术患者和患有炎症性肠病、慢性肝病或心力衰竭的患者中测量了血红蛋白浓度、总血红蛋白质量(优化的一氧化碳再呼吸法),并计算了血浆体积,从而探讨了这个问题。我们研究了 109 名参与者。血红蛋白质量与健康、手术和炎症性肠病组的浓度密切相关(r=0.687-0.871,<0.001)。然而,在肝病(r=0.410,=0.11)和心力衰竭患者中,相关性较差(r=0.312,=0.16)。在这里,血红蛋白质量解释了其浓度变化的一小部分(调整后的 R 值分别为 0.109 和 0.052;=0.11 和 0.16),而血浆体积则解释了大部分(在心脏病和肝病中 R 值分别变化 0.724 和 0.805,<0.0001)。具有相同(正常或升高)总血红蛋白质量的典型患者被诊断为严重贫血(或不贫血),这取决于未测量甚至未被视为原因的血浆体积差异。一般认为贫血通常反映血红蛋白缺乏的传统推论可能具有误导性,可能导致不适当的测试和治疗干预,以解决“血红蛋白缺乏”而不是“血浆体积过多”。目前,总血红蛋白质量和血浆体积的测量既简单、廉价又安全,提倡更常规地使用。