Haeusler Gabrielle M, Thursky Karin A, Mechinaud Francoise, Babl Franz E, De Abreu Lourenco Richard, Slavin Monica A, Phillips Robert
The Paediatric Integrated Cancer Service, 50 Flemington Road, Parkville, Victoria 3052, Australia.
Department of Infectious Diseases, Peter MacCallum Cancer Centre, 305 Grattan Street, Melbourne, Victoria 3000, Australia.
Br J Cancer. 2017 Jul 11;117(2):171-178. doi: 10.1038/bjc.2017.154. Epub 2017 Jun 13.
The aim of this study was to validate the 'Predicting Infectious ComplicatioNs in Children with Cancer' (PICNICC) clinical decision rule (CDR) that predicts microbiologically documented infection (MDI) in children with cancer and fever and neutropenia (FN). We also investigated costs associated with current FN management strategies in Australia.
Demographic, episode, outcome and cost data were retrospectively collected on 650 episodes of FN. We assessed the discrimination, calibration, sensitivity and specificity of the PICNICC CDR in our cohort compared with the derivation data set.
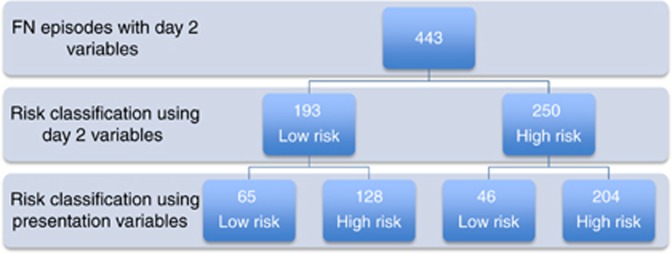
Using the original variable coefficients, the CDR performed poorly. After recalibration the PICNICC CDR had an area under the receiver operating characteristic (AUC-ROC) curve of 0.638 (95% CI 0.590-0.685) and calibration slope of 0.24. The sensitivity, specificity, positive predictive value and negative predictive value of the PICNICC CDR at presentation was 78.4%, 39.8%, 28.6% and 85.7%, respectively. For bacteraemia, the sensitivity improved to 85.2% and AUC-ROC to 0.71. Application at day 2, taking into consideration the proportion of MDI known (43%), further improved the sensitivity to 87.7%. Length of stay is the main contributor to cost of FN treatment, with an average cost per day of AUD 2183 in the low-risk group.
For prediction of any MDI, the PICNICC rule did not perform as well at presentation in our cohort as compared with the derivation study. However, for bacteraemia, the predictive ability was similar to that of the derivation study, highlighting the importance of recalibration using local data. Performance also improved after an overnight period of observation. Implementation of a low-risk pathway, using the PICNICC CDR after a short period of inpatient observation, is likely to be safe and has the potential to reduce health-care expenditure.
本研究的目的是验证“预测癌症患儿感染并发症”(PICNICC)临床决策规则(CDR),该规则用于预测患有癌症、发热且中性粒细胞减少(FN)的儿童发生微生物学确诊感染(MDI)的情况。我们还调查了澳大利亚当前FN管理策略的相关成本。
回顾性收集了650例FN病例的人口统计学、病程、结局和成本数据。我们将队列中PICNICC CDR的区分度、校准度、敏感性和特异性与推导数据集进行了比较。
使用原始变量系数时,CDR表现不佳。重新校准后,PICNICC CDR的受试者工作特征曲线下面积(AUC-ROC)为0.638(95%置信区间0.590-0.685),校准斜率为0.24。PICNICC CDR在初诊时的敏感性、特异性、阳性预测值和阴性预测值分别为78.4%、39.8%、28.6%和85.7%。对于菌血症,敏感性提高到85.2%,AUC-ROC提高到0.71。考虑到已知的MDI比例(43%),在第2天应用该规则进一步将敏感性提高到87.7%。住院时间是FN治疗成本的主要因素,低风险组的平均每日成本为2183澳元。
对于预测任何MDI,与推导研究相比,PICNICC规则在我们队列中的初诊表现不佳。然而,对于菌血症,预测能力与推导研究相似,突出了使用本地数据进行重新校准的重要性。经过一夜的观察期后,性能也有所改善。在短期住院观察后使用PICNICC CDR实施低风险路径可能是安全的,并且有可能减少医疗保健支出。