Hui Li, Jun-Bin Zhang, Xiao-Long Chen, Lei Fan, Li Wang, Shi-Hui Li, Yang Yang, Gui-Hua Chen, Gen-Shu Wang, Department of Hepatic Surgery and Liver Transplantation Center of the Third Affiliated Hospital, Organ Transplantation Institute, Sun Yat-Sen University, Guangzhou 510630, Guangdong Province, China.
World J Gastroenterol. 2017 May 28;23(20):3730-3743. doi: 10.3748/wjg.v23.i20.3730.
To perform a systematic review and meta-analysis on minimally conventional invasive techniques for harvesting grafts for living donor liver transplantation.
PubMed, Web of Science, EMBASE, and the Cochrane Library were searched comprehensively for studies comparing MILDH with conventional living donor hepatectomy (CLDH). Intraoperative and postoperative outcomes (operative time, estimated blood loss, postoperative liver function, length of hospital stay, analgesia use, complications, and survival rate) were analyzed in donors and recipients. Articles were included if they: (1) compared the outcomes of MILDH and CLDH; and (2) reported at least some of the above outcomes.
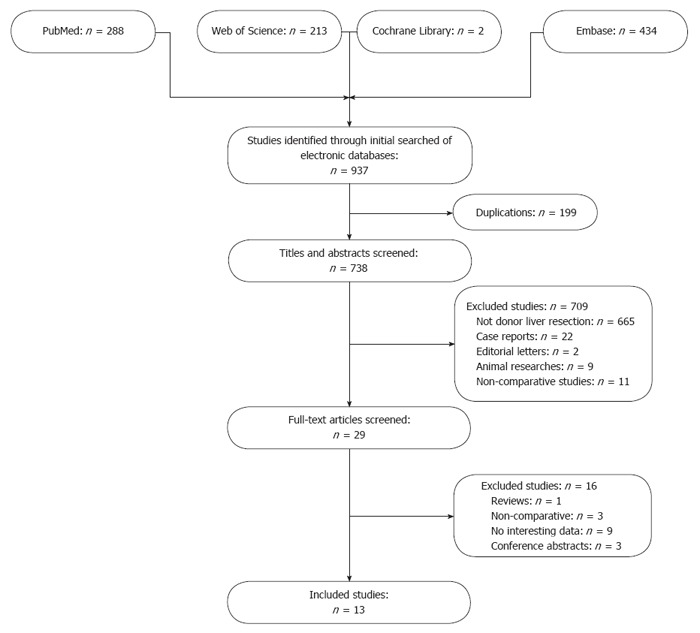
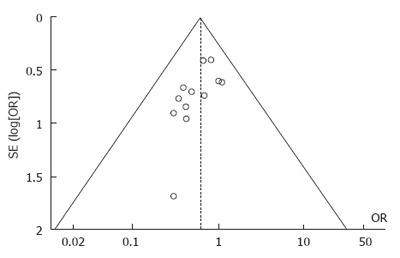
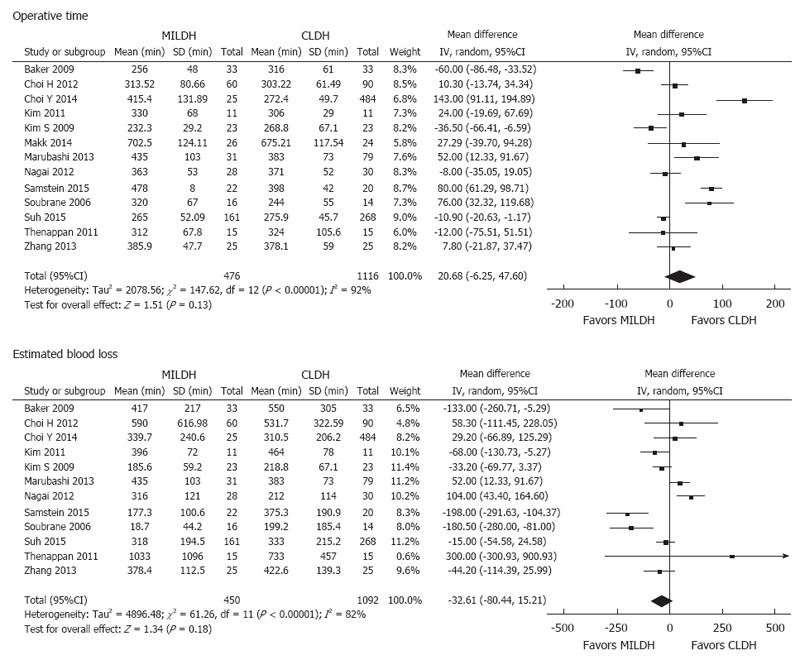
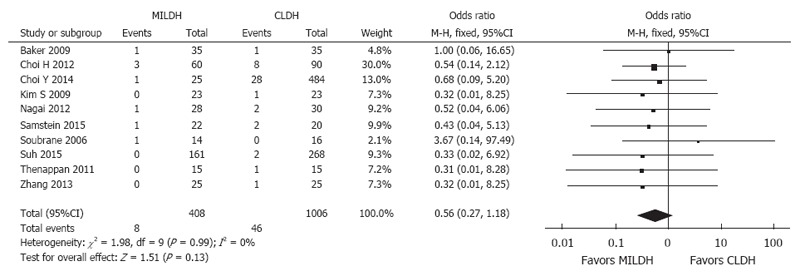
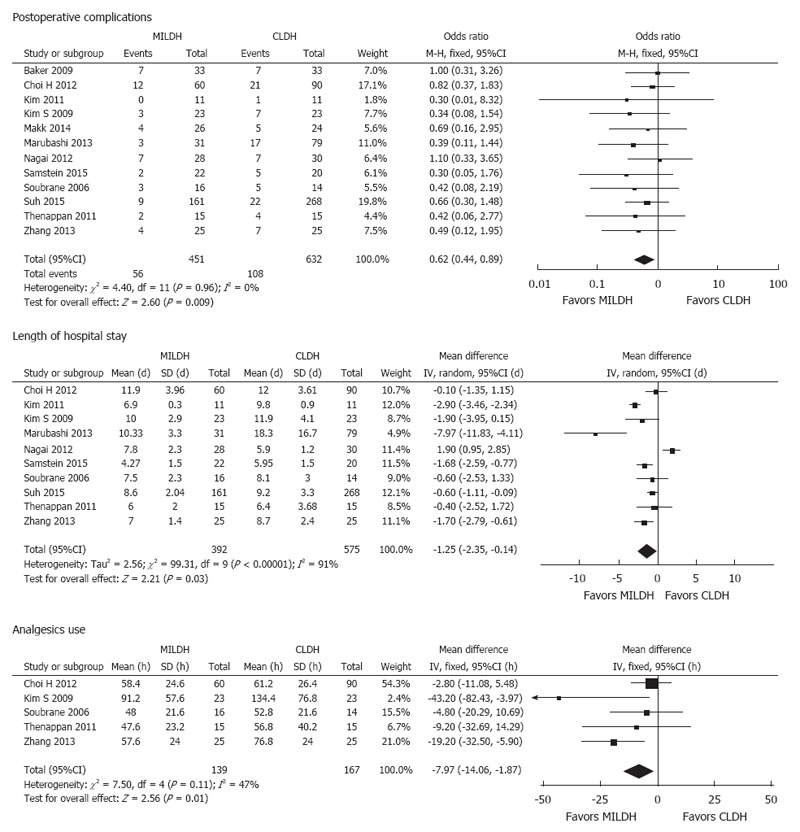
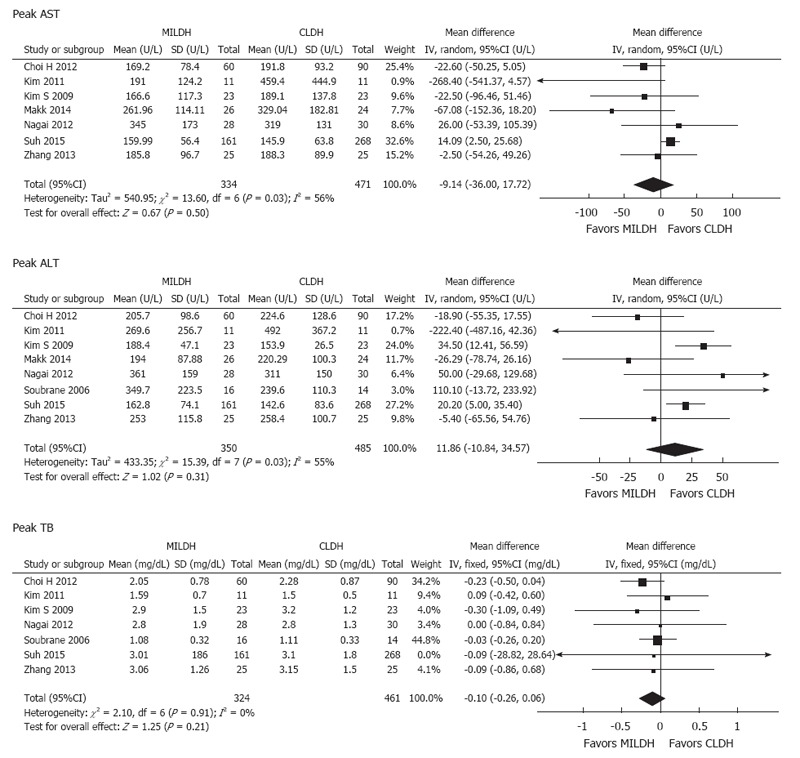
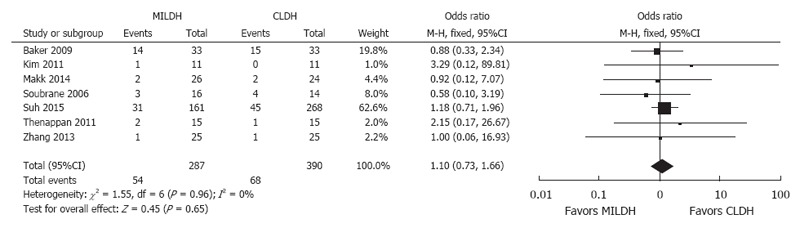
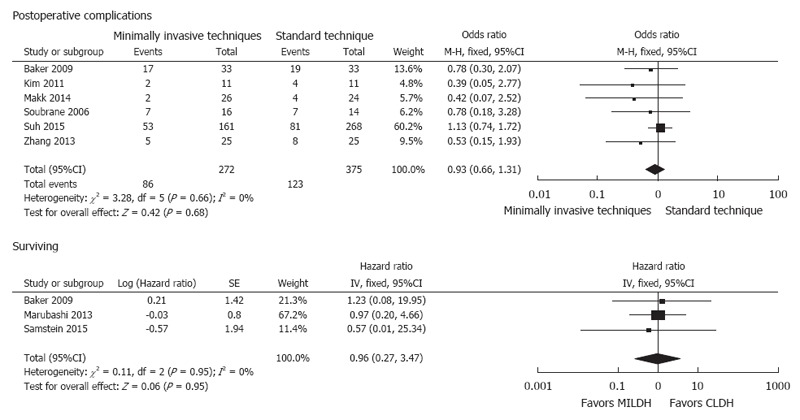
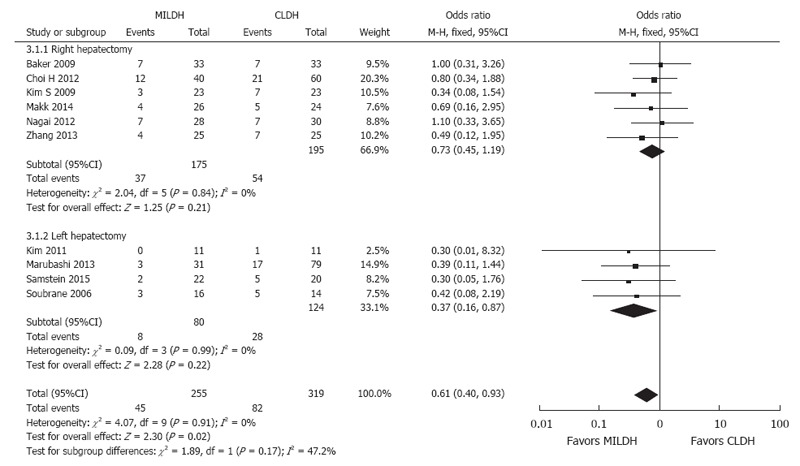
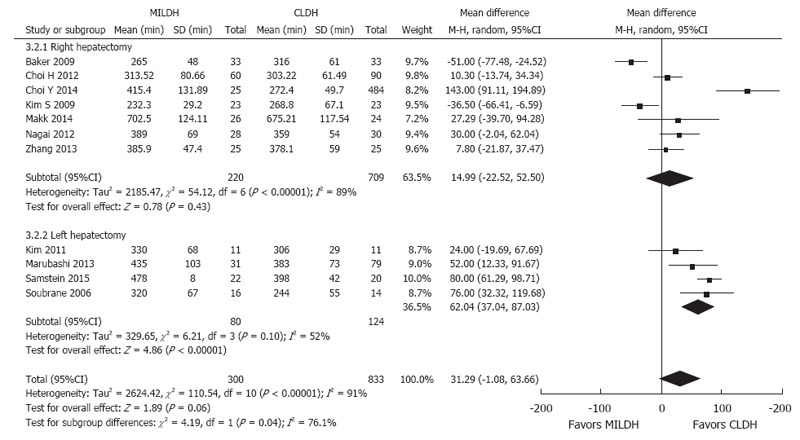
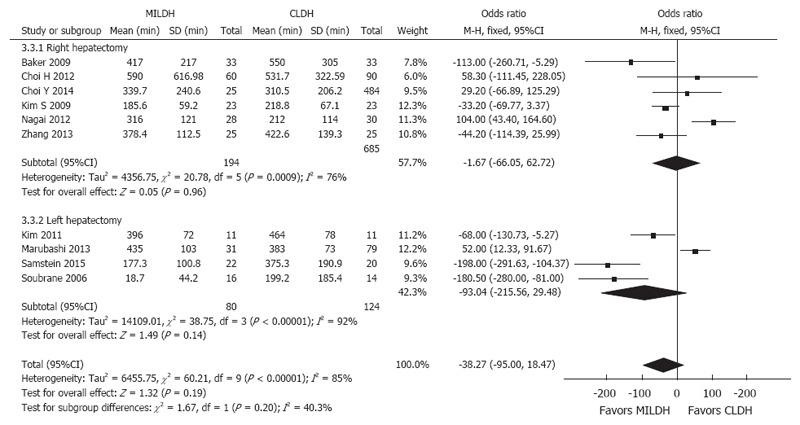
Of 937 articles identified, 13, containing 1592 patients, met our inclusion criteria and were included in the meta-analysis. For donors, operative time [weighted mean difference (WMD) = 20.68, 95%CI: -6.25-47.60, = 0.13] and blood loss (WMD = -32.61, 95%CI: -80.44-5.21, = 0.18) were comparable in the two groups. In contrast, analgesia use (WMD = -7.79, 95%CI: -14.06-1.87, = 0.01), postoperative complications [odds ratio (OR) = 0.62, 95%CI: 0.44-0.89, = 0.009], and length of hospital stay (WMD): -1.25, 95%CI: -2.35-0.14, = 0.03) significantly favored MILDH. No differences were observed in recipient outcomes, including postoperative complications (OR = 0.93, 95%CI: 0.66-1.31, = 0.68) and survival rate (HR = 0.96, 95%CI: 0.27-3.47, = 0.95). Funnel plot and statistical methods showed a low probability of publication bias.
MILDH is safe, effective, and feasible for living donor liver resection with fewer donor postoperative complications, reduced length of hospital stay and analgesia requirement than CLDH.
系统评价微创供肝获取技术(MILDH)与传统活体肝切除术(CLDH)治疗活体肝供者的效果。
全面检索 PubMed、Web of Science、EMBASE 和 Cochrane Library,比较 MILDH 与 CLDH 的研究。分析供者和受者术中及术后结局(手术时间、估计失血量、术后肝功能、住院时间、镇痛使用、并发症和生存率)。纳入符合以下标准的研究:(1)比较 MILDH 与 CLDH 结局;(2)报告至少上述部分结局。
共纳入 937 篇文献,其中 13 项研究(1592 例患者)符合纳入标准,纳入 meta 分析。供者中,MILDH 组的手术时间[加权均数差(WMD)=20.68,95%CI:-6.25-47.60, =0.13]和失血量[WMD=-32.61,95%CI:-80.44-5.21, =0.18]与 CLDH 组无显著差异。但 MILDH 组的镇痛药物使用率[WMD=-7.79,95%CI:-14.06-1.87, =0.01]、术后并发症[比值比(OR)=0.62,95%CI:0.44-0.89, =0.009]和住院时间[WMD=-1.25,95%CI:-2.35-0.14, =0.03]显著低于 CLDH 组。受者的术后并发症(OR=0.93,95%CI:0.66-1.31, =0.68)和生存率(HR=0.96,95%CI:0.27-3.47, =0.95)差异无统计学意义。漏斗图和统计学方法提示发表偏倚可能性低。
MILDH 安全、有效且可行,与 CLDH 相比,可减少供者术后并发症、缩短住院时间和减少镇痛药物需求。