Belete Hewan, Burns Linda J, Shanley Ryan, Nayar Manju, McClune Brian, Lazaryan Aleksandr, Bachanova Veronika, Bejanyan Nelli, Ustun Celalettin, Brunstein Claudio, Weisdorf Daniel J, Arora Mukta
Division of Hematology, University of Minnesota, Oncology and Transplantation, Minneapolis, Minnesota, 55455.
Health Services Research, National Marrow Donor Program, Minneapolis, Minnesota.
Am J Hematol. 2017 Sep;92(9):E529-E533. doi: 10.1002/ajh.24814. Epub 2017 Jul 19.
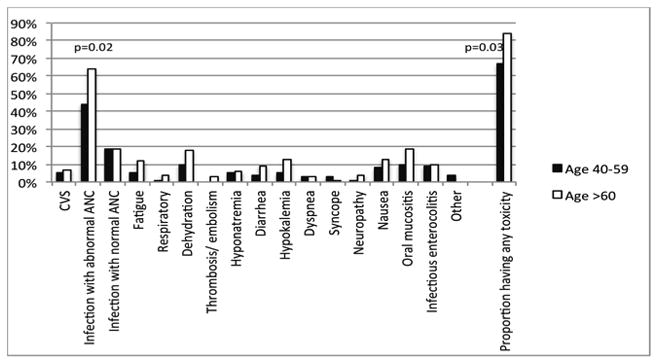
With advances in supportive care, autologous hematopoietic cell transplant (AHCT) is increasingly being performed for patients older than 60 years. We analyzed patients receiving an AHCT for multiple myeloma or lymphoma in a contemporary cohort (2010-2012), with consistent treatment and supportive care and compared outcomes [CTCAE grade 3-5 toxicities, nonrelapse mortality (NRM) and overall-survival (OS)] of younger (40-59 years, n = 77) versus older (≥60 years, n = 67) recipients. The proportion of patients with neutropenic infections was higher in the older group (64% vs. 44%; P = 0.02). The proportion of patients with any grade 3-5 toxicity was also higher in the older group (84% vs. 67%, P = 0.03). In multivariate analysis, older age was significantly associated with higher odds (OR: 2.57, 95% CI:1.09-6.05) of grade 3-5 toxicity. The NRM was 3% (older) vs. 0% (younger) at 1 year. The probability of OS at 2 years was lower in the older group (76% vs. 90%, P = 0.04). Though AHCT can be performed safely in older recipients, the higher toxicity and slightly higher NRM in this population needs attention. Studies focusing on risk-stratification in older patients would further help predict toxicity. Further studies addressing enhanced supportive care needs for older patients who are most likely to benefit are indicated.
随着支持性治疗的进展,自体造血细胞移植(AHCT)越来越多地应用于60岁以上的患者。我们分析了当代队列(2010 - 2012年)中接受AHCT治疗多发性骨髓瘤或淋巴瘤的患者,这些患者接受了一致的治疗和支持性护理,并比较了年轻(40 - 59岁,n = 77)与年长(≥60岁,n = 67)接受者的结局[美国国立癌症研究所通用毒性标准(CTCAE)3 - 5级毒性、非复发死亡率(NRM)和总生存期(OS)]。老年组中性粒细胞减少感染患者的比例更高(64%对44%;P = 0.02)。老年组3 - 5级任何毒性的患者比例也更高(84%对67%,P = 0.03)。在多变量分析中,年龄较大与3 - 5级毒性的较高几率显著相关(比值比:2.57,95%置信区间:1.09 - 6.05)。1年时NRM为3%(老年组)对0%(年轻组)。老年组2年时的OS概率较低(76%对90%,P = 0.04)。虽然AHCT可以在老年接受者中安全进行,但该人群中较高的毒性和略高的NRM需要关注。关注老年患者风险分层的研究将进一步有助于预测毒性。需要进一步开展研究,以满足最有可能受益的老年患者对强化支持性护理的需求。