Department of Population Sciences, City of Hope, Duarte, CA, USA.
Department of Hematology and Hematopoietic Cell Transplantation, City of Hope, Duarte, CA, USA.
J Cachexia Sarcopenia Muscle. 2020 Aug;11(4):962-972. doi: 10.1002/jcsm.12570. Epub 2020 Mar 25.
The number of patients undergoing autologous haematopoietic cell transplant (HCT) is growing, but little is known about the factors that predict adverse outcomes. Low muscle mass and obesity are associated with disability and premature mortality in individuals with non-malignant diseases and may predict outcomes after autologous HCT.
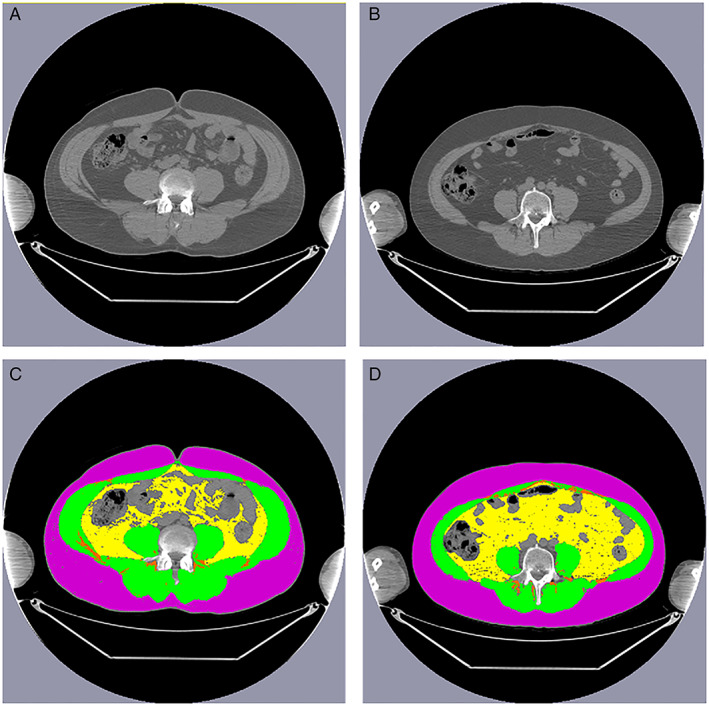
This was a retrospective cohort study of 320 patients who underwent autologous HCT for Hodgkin or non-Hodgkin lymphoma between 2009 and 2014. Sarcopenia {skeletal muscle index male: <43 cm/m [body mass index (BMI) < 25 kg/m ] or < 53 cm/m [BMI ≥ 25 kg/m ] and female: <41 cm/m [regardless of BMI]) and obesity [total abdominal adiposity ≥450.0 cm (male), ≥396.4 cm (female)] were assessed from single-slice abdominal pre-HCT computed tomography images. Length of hospital stay, first unplanned intensive care unit admission, and 30-day unplanned readmission were evaluated based on body composition using multivariable regression analysis, and mortality was evaluated with Kaplan-Meier analysis and Gray's test.
Median age at HCT was 53.3 years (range, 18.5 to 78.1 years); 26.3% were sarcopenic and an additional 7.8% were sarcopenic obese pre-HCT. Sarcopenic obesity was associated with increased risk of prolonged hospitalization [odds ratio (OR) = 3.6, 95% confidence interval (CI) 1.3-9.8], intensive care unit admission (OR = 4.7, 95% CI 1.5-16.1), and unplanned readmission after HCT (OR = 13.6, 95% CI 2.5-62.8). Patients who were sarcopenic obese also had the highest mortality risk at 1 year [hazard ratio (HR): 3.9, 95% CI 1.1-11.0] and 5 years (HR: 2.5, 95% CI 1.1-5.5), compared with patients with normal body composition. Sarcopenia alone, but not obesity alone, was associated with an increased risk of these outcomes, albeit with a lower magnitude of risk than in patients who were sarcopenic obese.
Sarcopenic obesity was an important predictor of outcomes in patients undergoing autologous HCT. These findings could inform targeted prevention strategies in patients at highest risk of complications after HCT.
接受自体造血细胞移植(HCT)的患者数量正在增加,但人们对预测不良结局的因素知之甚少。肌肉减少症和肥胖与非恶性疾病患者的残疾和过早死亡有关,并且可能预测自体 HCT 后的结局。
这是一项回顾性队列研究,共纳入 320 例 2009 年至 2014 年间因霍奇金或非霍奇金淋巴瘤接受自体 HCT 的患者。使用术前单次腹部 CT 图像评估肌肉减少症(男性:<43 cm/m[BMI<25 kg/m ]或<53 cm/m[BMI≥25 kg/m ];女性:<41 cm/m[无论 BMI 如何])和肥胖症[总腹部脂肪≥450.0 cm(男性),≥396.4 cm(女性)]。使用多变量回归分析,根据体成分评估住院时间、首次计划外重症监护病房入院和 30 天内计划外再入院,使用 Kaplan-Meier 分析和 Gray 检验评估死亡率。
HCT 时的中位年龄为 53.3 岁(范围 18.5 岁至 78.1 岁);26.3%的患者术前存在肌肉减少症,另有 7.8%的患者术前存在肌肉减少症合并肥胖症。肌肉减少症合并肥胖症与住院时间延长(优势比[OR] = 3.6,95%置信区间[CI] 1.3-9.8)、重症监护病房入院(OR = 4.7,95% CI 1.5-16.1)和 HCT 后计划外再入院(OR = 13.6,95% CI 2.5-62.8)的风险增加相关。与体成分正常的患者相比,肌肉减少症合并肥胖症患者的 1 年(风险比[HR]:3.9,95% CI 1.1-11.0)和 5 年(HR:2.5,95% CI 1.1-5.5)死亡率风险最高。单纯肌肉减少症而不是单纯肥胖症与这些结局的风险增加相关,但其风险程度低于肌肉减少症合并肥胖症患者。
肌肉减少症合并肥胖症是接受自体 HCT 患者结局的重要预测指标。这些发现可以为 HCT 后并发症风险最高的患者提供有针对性的预防策略。