Rahmel Tim, Asmussen Sven, Karlik Jan, Steinmann Jörg, Adamzik Michael, Peters Jürgen
Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie, Universitätsklinikum Knappschaftskrankenhaus Bochum, In der Schornau 23-25, D-44892, Bochum, Germany.
Klinik für Anästhesiologie und Intensivmedizin, Universität Duisburg-Essen and Universitätsklinikum Essen, D-45122, Essen, Germany.
BMC Anesthesiol. 2017 Jun 14;17(1):78. doi: 10.1186/s12871-017-0376-5.
We tested the hypothesis that moxifloxacin monotherapy is equally effective and safe as a betalactam antibiotic based combination therapy in patients with acute respiratory distress syndrome (ARDS) evoked by severe community acquired pneumonia (CAP).
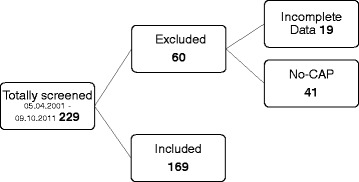
In a retrospective chart review study of 229 patients with adult respiratory distress syndrome (ARDS) admitted to our intensive care unit between 2001 and 2011, 169 well-characterized patients were identified to suffer from severe CAP. Patients were treated with moxifloxacin alone, moxifloxacin in combination with ß-lactam antibiotics, or with another antibiotic regimen based on ß-lactam antibiotics, at the discretion of the admitting attending physician. The primary endpoint was 30-day survival. To assess potential drug-induced liver injury, we also analyzed biomarkers of liver cell integrity.
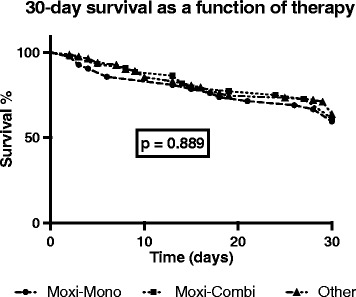
30-day survival (69% overall) did not differ (p = 0.89) between moxifloxacin monotherapy (n = 42), moxifloxacin combination therapy (n = 44), and other antibiotic treatments (n = 83). We found significantly greater maximum activity of aspartate transaminase (p = 0.048), alanine aminotransferase (p = 0.003), and direct bilirubin concentration (p = 0.01) in the moxifloxacin treated groups over the first 10-20 days. However, these in-between group differences faded over time, and no differences remained during the last 10 days of observation.
In CAP evoked ARDS, moxifloxacin monotherapy and moxifloxacin combination therapy was not different to a betalactam based antibiotic regimen with respect to 30-day mortality, and temporarily increased markers of liver cell integrity had no apparent clinical impact. Thus, in contrast to the current S3 guidelines, moxifloxacin may also be safe and effective even in patients with severe CAP evoked ARDS while providing coverage of an extended spectrum of severe CAP evoking bacteria. However, further prospective studies are needed for definite recommendations.
我们检验了如下假设:在因严重社区获得性肺炎(CAP)引发急性呼吸窘迫综合征(ARDS)的患者中,莫西沙星单药治疗与基于β-内酰胺类抗生素的联合治疗同样有效且安全。
在一项对2001年至2011年间入住我们重症监护病房的229例成人呼吸窘迫综合征(ARDS)患者的回顾性病历审查研究中,确定169例特征明确的患者患有严重CAP。由主治医生酌情决定,患者接受单独的莫西沙星治疗、莫西沙星与β-内酰胺类抗生素联合治疗或基于β-内酰胺类抗生素的其他抗生素治疗方案。主要终点是30天生存率。为评估潜在的药物性肝损伤,我们还分析了肝细胞完整性的生物标志物。
莫西沙星单药治疗组(n = 42)、莫西沙星联合治疗组(n = 44)和其他抗生素治疗组(n = 83)的30天生存率(总体为69%)无差异(p = 0.89)。我们发现,在最初的10至20天内,莫西沙星治疗组的天冬氨酸转氨酶最大活性(p = 0.048)、丙氨酸转氨酶(p = 0.003)和直接胆红素浓度(p = 0.01)显著更高。然而,这些组间差异随时间逐渐消失,在观察的最后10天内不再有差异。
在CAP诱发的ARDS中,莫西沙星单药治疗和莫西沙星联合治疗在30天死亡率方面与基于β-内酰胺类的抗生素治疗方案无差异,且肝细胞完整性标志物的暂时升高没有明显的临床影响。因此,与当前的S3指南相反,即使在严重CAP诱发ARDS的患者中,莫西沙星也可能是安全有效的,同时能覆盖引起严重CAP的多种细菌。然而,需要进一步的前瞻性研究以给出明确建议。