Enomoto Hiroyuki, Fujikoshi Shinji, Funai Jumpei, Sasaki Nao, Ossipov Michael H, Tsuji Toshinaga, Alev Levent, Ushida Takahiro
Medical Science, Eli Lilly Japan K.K., Tokyo.
Statistical Science.
J Pain Res. 2017 Jun 1;10:1357-1368. doi: 10.2147/JPR.S133396. eCollection 2017.
Comorbid depression and depressive symptoms are common in patients with chronic low back pain (CLBP). Duloxetine is clinically effective in major depressive disorder and several chronic pain states, including CLBP. The objective of this post hoc meta-analysis was to assess direct and indirect analgesic efficacy of duloxetine for patients with CLBP in previous clinical trials.
Post hoc path analyses were conducted of 3 randomized, double-blind, clinical studies of patients receiving duloxetine or placebo for CLBP. The primary outcome measure for pain was the Brief Pain Inventory, average pain score. A secondary outcome measure, the Beck Depression Inventory-II, was used for depressive symptoms. The changes in score from baseline to endpoint were determined for each index. Path analyses were employed to calculate the proportion of analgesia that may be attributed to a direct effect of duloxetine on pain.
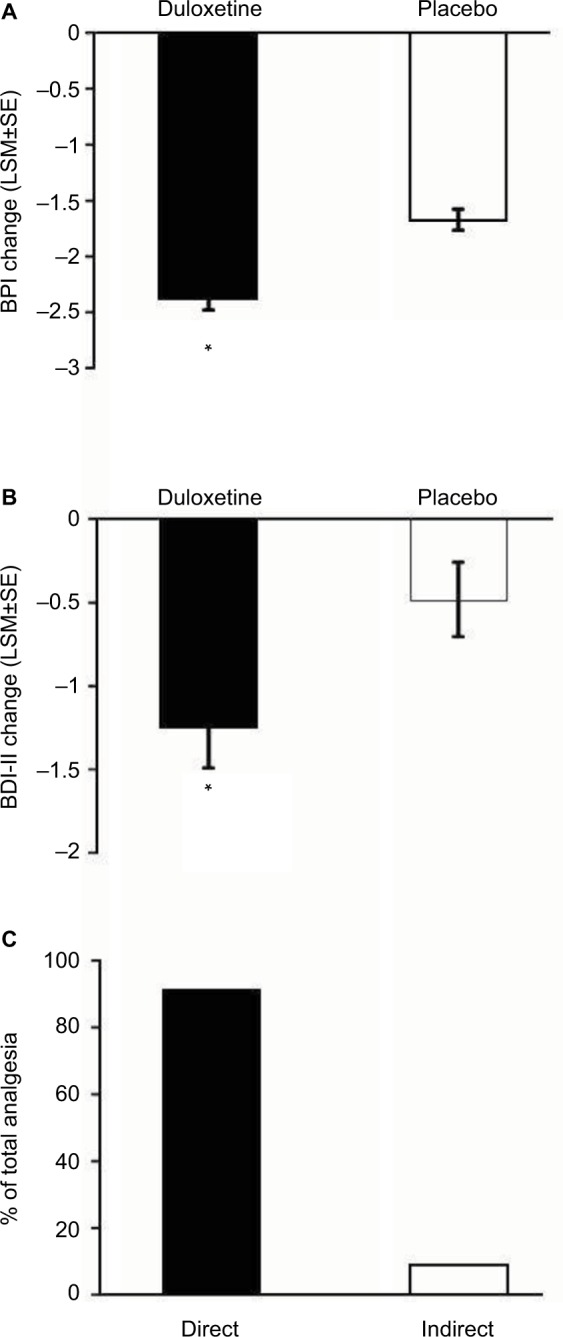
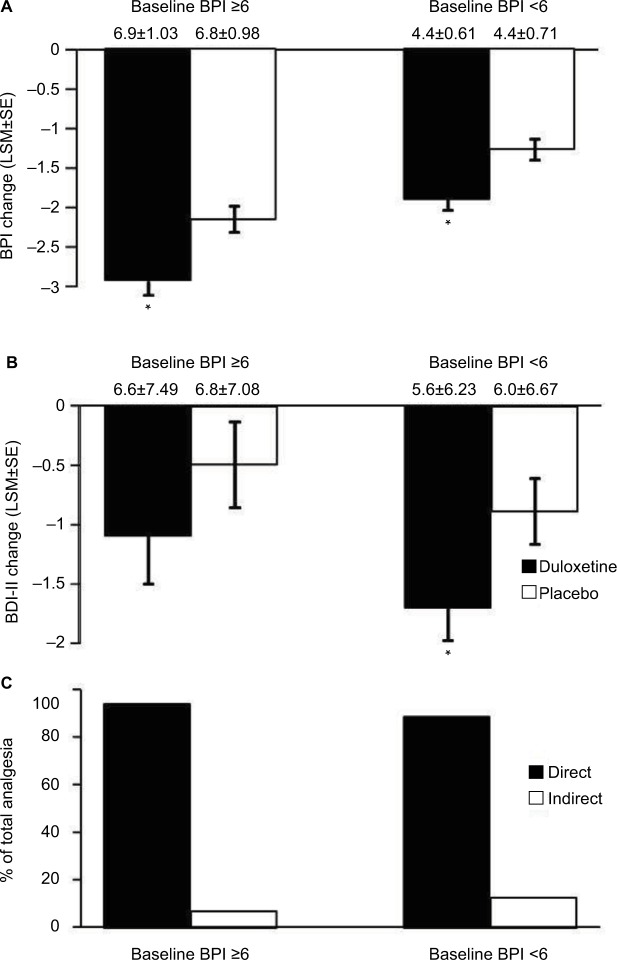
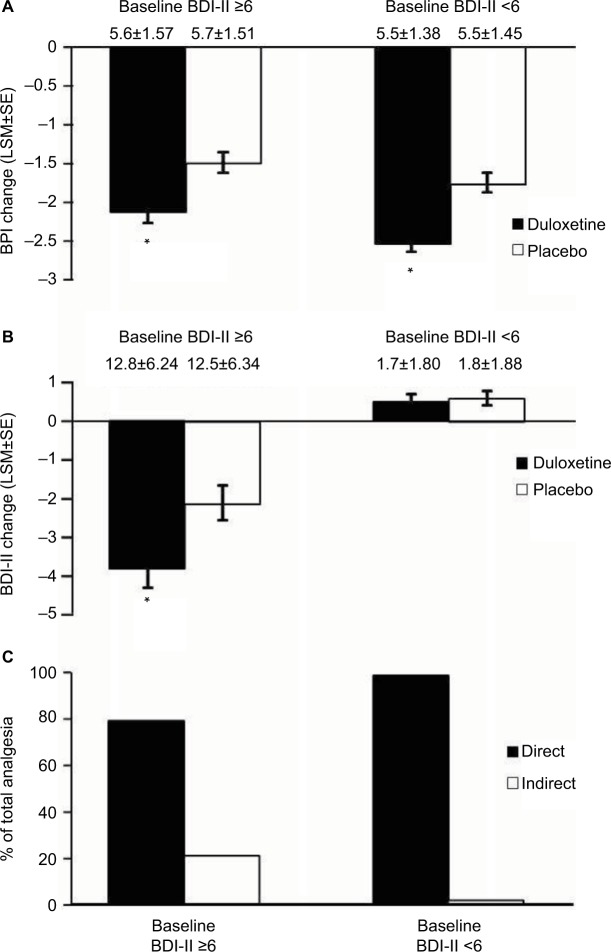
A total of 851 patients (400 duloxetine and 451 placebo) were included in this analysis. Duloxetine significantly improved pain scores compared with placebo (<0.001). It also significantly improved depressive scores compared with placebo (=0.015). Path analyses showed that 91.1% of the analgesic effect of duloxetine could be attributed to a direct analgesic effect, and 8.9% to its antidepressant effect. Similar results were obtained when data were evaluated at weeks 4 and 7, and when patients were randomized to subgroups based on baseline pain scores, baseline depressive symptoms scores, and gender.
Duloxetine significantly improved pain in patients with CLBP. Path analyses results suggest that duloxetine produced analgesia mainly through mechanisms directly impacting pain modulation rather than lifting depressive symptoms. This effect was consistent across all subgroups tested.
合并抑郁症及抑郁症状在慢性下腰痛(CLBP)患者中很常见。度洛西汀在重度抑郁症及包括CLBP在内的几种慢性疼痛状态中具有临床疗效。这项事后荟萃分析的目的是评估在之前的临床试验中度洛西汀对CLBP患者的直接和间接镇痛效果。
对3项关于CLBP患者接受度洛西汀或安慰剂治疗的随机、双盲临床研究进行事后路径分析。疼痛的主要结局指标是简明疼痛量表的平均疼痛评分。次要结局指标是贝克抑郁量表第二版,用于评估抑郁症状。确定每个指标从基线到终点的评分变化。采用路径分析计算度洛西汀对疼痛直接作用所致镇痛的比例。
本分析共纳入851例患者(400例度洛西汀组和451例安慰剂组)。与安慰剂相比,度洛西汀显著改善了疼痛评分(<0.001)。与安慰剂相比,它还显著改善了抑郁评分(=0.015)。路径分析显示,度洛西汀的镇痛作用91.1%可归因于直接镇痛作用,8.9%归因于其抗抑郁作用。在第4周和第7周评估数据时,以及根据基线疼痛评分、基线抑郁症状评分和性别将患者随机分组时,均得到了类似结果。
度洛西汀显著改善了CLBP患者的疼痛。路径分析结果表明,度洛西汀产生镇痛作用主要是通过直接影响疼痛调节的机制,而非缓解抑郁症状。在所有测试的亚组中,这种效果都是一致的。