Alev Levent, Fujikoshi Shinji, Yoshikawa Aki, Enomoto Hiroyuki, Ishida Mitsuhiro, Tsuji Toshinaga, Ogawa Kei, Konno Shinichi
Bio-Medicine.
Statistical Science.
J Pain Res. 2017 Jul 24;10:1723-1731. doi: 10.2147/JPR.S138297. eCollection 2017.
Duloxetine has demonstrated efficacy in chronic low back pain (CLBP). We examined the predictors of response to duloxetine for CLBP.
This was a post hoc analysis of pooled data from 4 double-blind, ran-domized, placebo-controlled trials of duloxetine (60 mg/day for 12-14 weeks) in adult patients with CLBP. Primary outcome was proportion of patients with ≥30% reduction in Brief Pain Inventory (BPI) average pain ("pain reduction") at 12-14 weeks. The proportion of patients with ≥30% and ≥50% (secondary outcome) pain reduction in duloxetine and placebo groups was compared. Variables for responder analyses were early improvement (≥15% pain reduction at Week 2), sex, age, baseline BPI average pain score, duration of CLBP, and number of painful body sites according to the Michigan Body Map (≥2 vs 1 [isolated CLBP]; 1 trial); relative risk (RR) and 95% confidence interval (CI) were calculated.
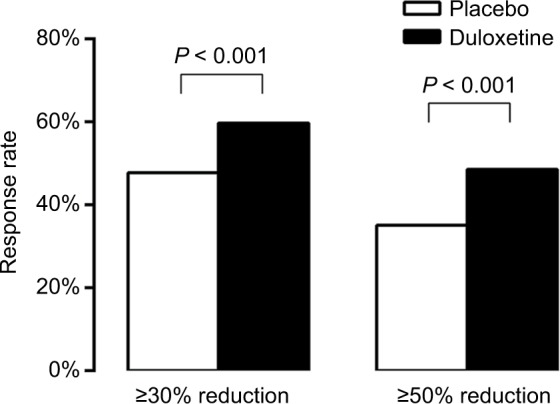
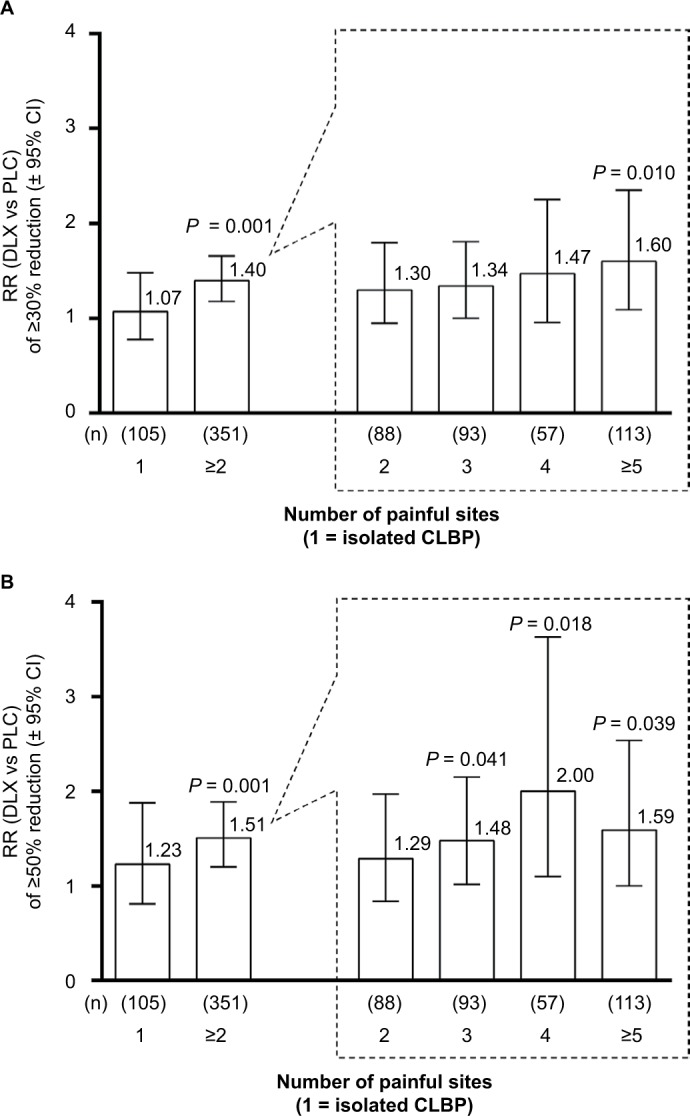
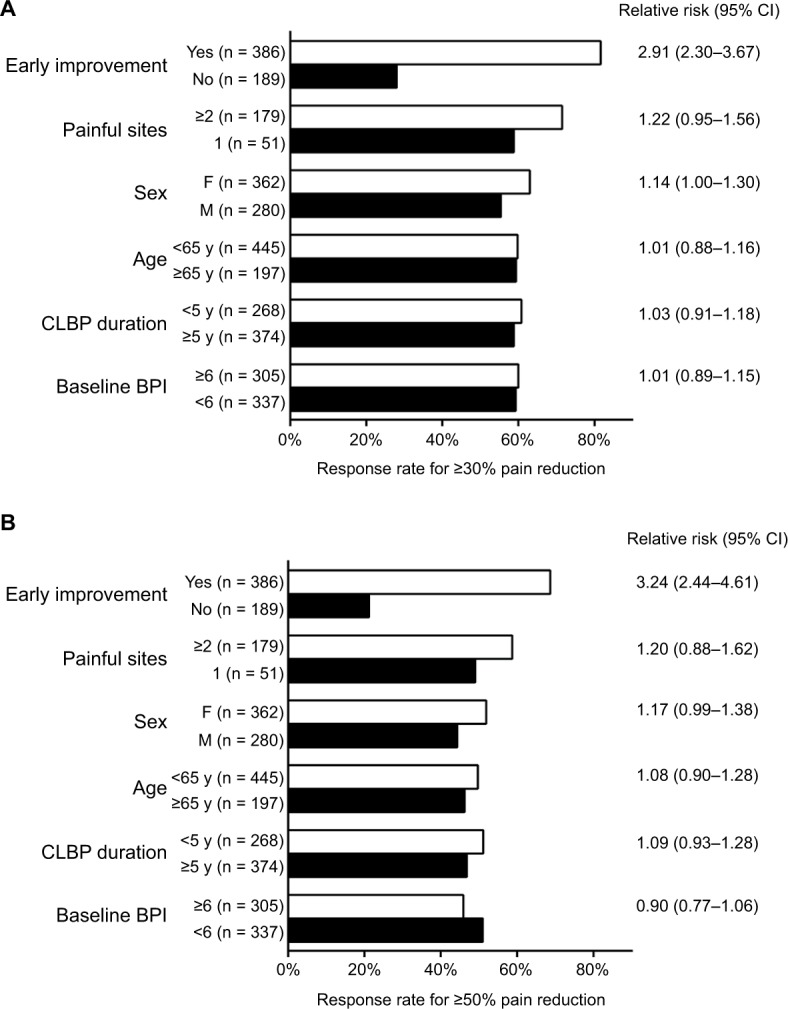
Compared with placebo (n = 653), a greater proportion of duloxetine-treated patients (n = 642) achieved ≥30% (59.7% vs 47.8%; < 0.001) and ≥50% pain reduction (48.6% vs 35.1%; < 0.001). Among duloxetine-treated patients, early improvement was associated with greater likelihood of ≥30% (RR [95% CI], 2.91 [2.30-3.67]) or ≥50% (3.24 [2.44-4.31]) pain reduction. Women were slightly more likely than men to achieve ≥30% (RR [95% CI], 1.14 [1.00-1.30]) or ≥50% (1.17 [0.99-1.38]) pain reduction. Response rates were similar between age, CLBP duration, and baseline BPI average pain score subgroups. Patients with ≥2 painful sites were more likely to respond to duloxetine 60 mg relative to placebo than patients with isolated CLBP (RR, duloxetine vs placebo [95% CI]: ≥30% reduction, ≥2 painful sites 1.40 [1.18-1.66], isolated CLBP 1.07 [0.78-1.48]; ≥50% reduction, ≥2 painful sites 1.51 [1.20-1.89], isolated CLBP 1.23 [0.81-1.88]).
Early pain reduction was indicative of overall response. Patients with multiple painful sites had more benefit from duloxetine than patients with isolated CLBP.
度洛西汀已被证明对慢性下腰痛(CLBP)有效。我们研究了度洛西汀治疗CLBP疗效的预测因素。
这是一项对4项度洛西汀(60毫克/天,持续12 - 14周)治疗成年CLBP患者的双盲、随机、安慰剂对照试验的汇总数据进行的事后分析。主要结局是在12 - 14周时简短疼痛量表(BPI)平均疼痛程度降低≥30%(“疼痛减轻”)的患者比例。比较了度洛西汀组和安慰剂组中疼痛减轻≥30%和≥50%(次要结局)的患者比例。反应者分析的变量包括早期改善(第2周时疼痛减轻≥15%)、性别、年龄、基线BPI平均疼痛评分、CLBP持续时间以及根据密歇根身体图谱划分的疼痛身体部位数量(≥2个部位与1个部位[孤立性CLBP];1项试验);计算相对风险(RR)和95%置信区间(CI)。
与安慰剂组(n = 653)相比,更多接受度洛西汀治疗的患者(n = 642)实现了≥30%(59.7%对47.8%;P < 0.001)和≥50%的疼痛减轻(48.6%对35.1%;P < 0.001)。在接受度洛西汀治疗的患者中,早期改善与疼痛减轻≥30%(RR[95%CI],2.91[2.30 - 3.67])或≥50%(3.24[2.44 - 4.31])的可能性更大相关。女性比男性更有可能实现≥30%(RR[95%CI],1.14[1.00 - 1.30])或≥50%(1.17[0.99 - 1.38])的疼痛减轻。年龄、CLBP持续时间和基线BPI平均疼痛评分亚组之间的反应率相似。与孤立性CLBP患者相比,有≥2个疼痛部位的患者对60毫克度洛西汀的反应相对于安慰剂更明显(RR,度洛西汀与安慰剂[95%CI]:≥30%减轻,≥2个疼痛部位1.40[1.18 - 1.66],孤立性CLBP 1.07[0.78 - 1.48];≥50%减轻,≥2个疼痛部位1.51[1.20 - 1.89],孤立性CLBP 1.23[0.81 - 1.88])。
早期疼痛减轻表明总体反应情况。有多个疼痛部位的患者比孤立性CLBP患者从度洛西汀治疗中获益更多。