Vasudevan Pradeep, Powell Corrina, Nicholas Adeline K, Scudamore Ian, Greening James, Park Soo-Mi, Schoenmakers Nadia
Leicester Clinical Genetics, Women's and Children's Services, Leicester Royal Infirmary, LeicesterUK.
University of Cambridge Metabolic Research Laboratories, Wellcome Trust-Medical Research Council Institute of Metabolic Science, Addenbrooke's Hospital, CambridgeUK.
Endocrinol Diabetes Metab Case Rep. 2017 Jun 7;2017. doi: 10.1530/EDM-17-0040. eCollection 2017.
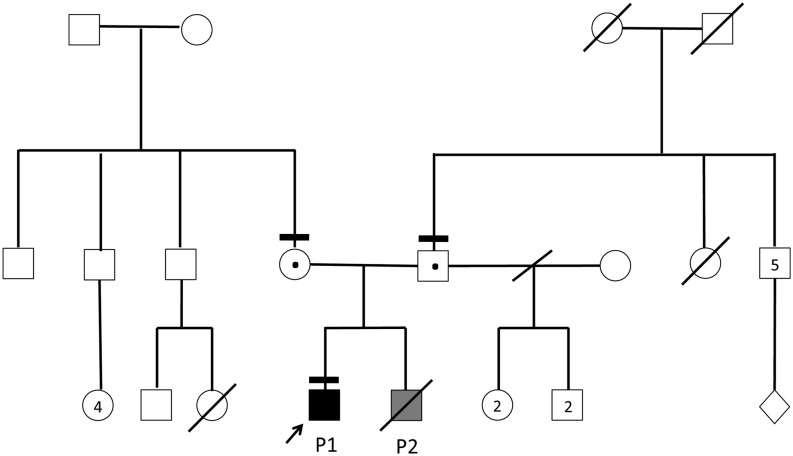
In the absence of maternal thyroid disease or iodine deficiency, fetal goitre is rare and usually attributable to dyshormonogenesis, for which genetic ascertainment is not always undertaken in the UK. Mechanical complications include tracheal and oesophageal compression with resultant polyhydramnios, malpresentation at delivery and neonatal respiratory distress. We report an Indian kindred in which the proband (first-born son) had congenital hypothyroidism (CH) without obvious neonatal goitre. His mother's second pregnancy was complicated by fetal hypothyroid goitre and polyhydramnios, prompting amniotic fluid drainage and intraamniotic therapy (with liothyronine, T3 and levothyroxine, T4). Sadly, intrauterine death occurred at 31 weeks. Genetic studies in the proband demonstrated compound heterozygous novel (c.5178delT, p.A1727Hfs*26) and previously described (c.7123G > A, p.G2375R) thyroglobulin () mutations which are the likely cause of fetal goitre in the deceased sibling. mutations rarely cause fetal goitre, and management remains controversial due to the potential complications of intrauterine therapy however an amelioration in goitre size may be achieved with intraamniotic T4, and intraamniotic T3/T4 combination has achieved a favourable outcome in one case. A conservative approach, with surveillance, elective delivery and commencement of levothyroxine neonatally may also be justified, although intubation may be required post delivery for respiratory obstruction. Our observations highlight the lethality which may be associated with fetal goitre. Additionally, although this complication may recur in successive pregnancies, our case highlights the possibility of discordance for fetal goitre in siblings harbouring the same dyshormonogenesis-associated genetic mutations. Genetic ascertainment may facilitate prenatal diagnosis and assist management in familial cases.
CH due to biallelic, loss-of-function mutations is well-described and readily treatable in childhood however mechanical complications from associated fetal goitre may include polyhydramnios, neonatal respiratory compromise and neck hyperextension with dystocia complicating delivery.CH due to mutations may manifest with variable phenotypes, even within the same kindred.Treatment options for hypothyroid dyshormogenic fetal goitre in a euthyroid mother include intraamniotic thyroid hormone replacement in cases with polyhydramnios or significant tracheal obstruction. Alternatively, cases may be managed conservatively with radiological surveillance, elective delivery and neonatal levothyroxine treatment, although intubation and ventilation may be required to support neonatal respiratory compromise.Genetic ascertainment in such kindreds may enable prenatal diagnosis and anticipatory planning for antenatal management of further affected offspring.
在没有母体甲状腺疾病或碘缺乏的情况下,胎儿甲状腺肿很少见,通常归因于激素合成障碍,在英国,对此并不总是进行基因鉴定。机械性并发症包括气管和食管受压,继而导致羊水过多、分娩时胎位异常及新生儿呼吸窘迫。我们报告了一个印度家族,先证者(长子)患有先天性甲状腺功能减退症(CH),无明显的新生儿甲状腺肿。他母亲的第二次妊娠因胎儿甲状腺功能减退性甲状腺肿和羊水过多而复杂化,促使进行羊水引流和羊膜腔内治疗(使用三碘甲状腺原氨酸、T3和左甲状腺素、T4)。遗憾的是,妊娠31周时发生了宫内死亡。对先证者的基因研究显示,存在复合杂合的新突变(c.5178delT,p.A1727Hfs*26)和先前描述的(c.7123G>A,p.G2375R)甲状腺球蛋白()突变,这些突变可能是已故同胞胎儿甲状腺肿的原因。甲状腺球蛋白突变很少导致胎儿甲状腺肿,由于宫内治疗存在潜在并发症,其管理仍存在争议,然而羊膜腔内注射T4可使甲状腺肿大小有所改善,并且羊膜腔内注射T3/T4联合治疗在1例中取得了良好效果。一种保守的方法,包括监测、择期分娩和新生儿期开始使用左甲状腺素也是合理的,尽管分娩后可能需要插管以解除呼吸道梗阻。我们的观察结果突出了与胎儿甲状腺肿相关的致死性。此外,尽管这种并发症可能在连续妊娠中复发,但我们的病例突出了携带相同激素合成障碍相关基因突变的同胞胎儿甲状腺肿不一致的可能性。基因鉴定可能有助于产前诊断并协助家族性病例的管理。
双等位基因功能丧失性甲状腺球蛋白突变导致的CH在儿童期已有充分描述且易于治疗,然而相关胎儿甲状腺肿引起的机械性并发症可能包括羊水过多、新生儿呼吸功能不全以及颈部过度伸展伴难产使分娩复杂化。甲状腺球蛋白突变导致的CH可能表现出不同的表型,即使在同一家族中也是如此。甲状腺功能正常的母亲体内甲状腺功能减退性激素合成障碍性胎儿甲状腺肿的治疗选择包括对羊水过多或有明显气管梗阻的病例进行羊膜腔内甲状腺激素替代治疗。或者,对于病例可采用保守治疗,进行放射学监测、择期分娩和新生儿左甲状腺素治疗,尽管可能需要插管和通气以支持新生儿呼吸功能不全。对此类家族进行基因鉴定可能有助于产前诊断,并为进一步受影响后代的产前管理进行前瞻性规划。