Zeh Clement, Ndiege Kenneth, Inzaule Seth, Achieng Rebecca, Williamson John, Chih-Wei Chang Joy, Ellenberger Dennis, Nkengasong John
Division of HIV/AIDS Prevention, U.S. Centers for Disease Control and Prevention, Kisumu, Kenya.
Centre for Global Health Research, Kenya Medical Research Institute, Kisumu, Kenya.
PLoS One. 2017 Jun 16;12(6):e0179316. doi: 10.1371/journal.pone.0179316. eCollection 2017.
Routine HIV viral load testing is not widely accessible in most resource-limited settings, including Kenya. To increase access to viral load testing, alternative sample types like dried blood spots (DBS), which overcome the logistic barriers associated with plasma separation and cold chain shipment need to be considered and evaluated. The current study evaluated matched dried blood spots (DBS) and dried plasma spots (DPS) against plasma using the Abbott M 2000 (Abbott) and Roche Cobas Ampliprep/Cobas TaqMan (CAP/CTM) quantitative viral load assays in western Kenya.
Matched plasma DBS and DPS were obtained from 200 HIV-1 infected antiretroviral treatment (ART)-experienced patients attending patient support centers in Western Kenya. Standard quantitative assay performance parameters with accompanying 95% confidence intervals (CI) were assessed at the assays lower detection limit (400cps/ml for CAP/CTM and 550cps/ml for Abbott) using SAS version 9.2. Receiver operating curves (ROC) were further used to assess viral-load thresholds with best assay performance (reference assay CAP/CTM plasma).
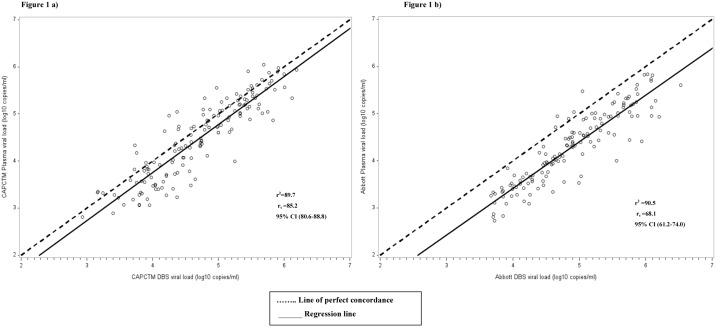
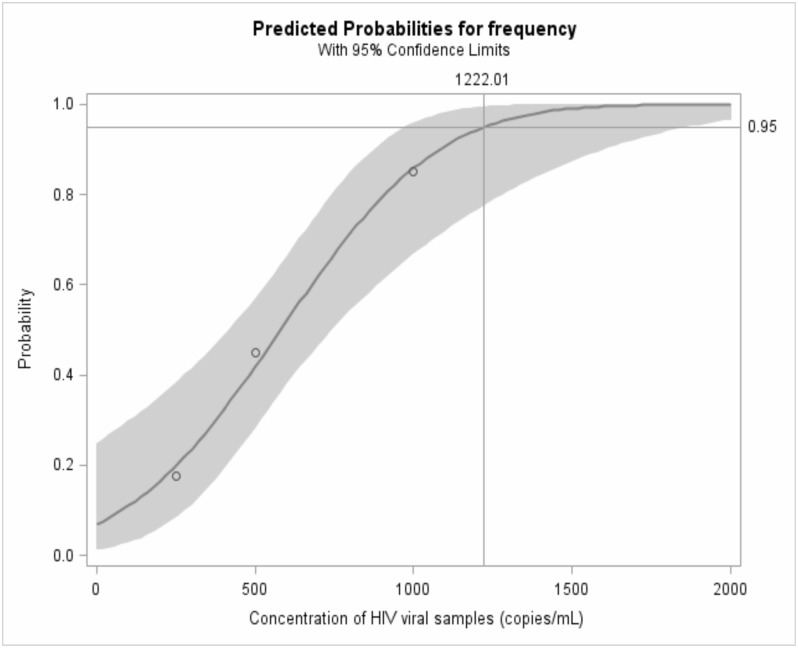
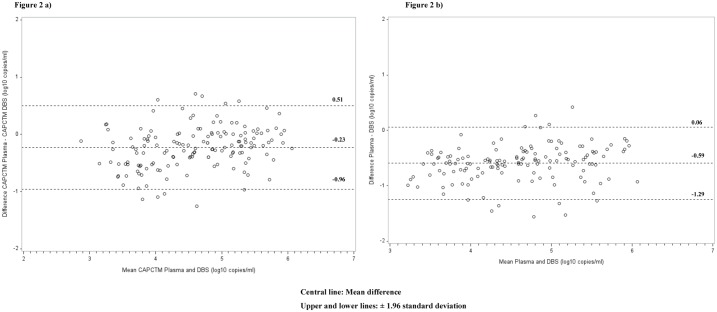
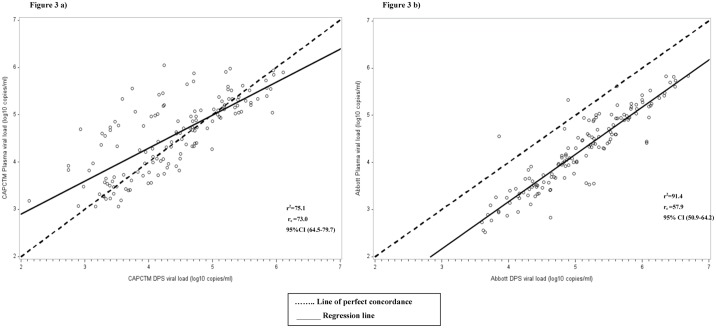
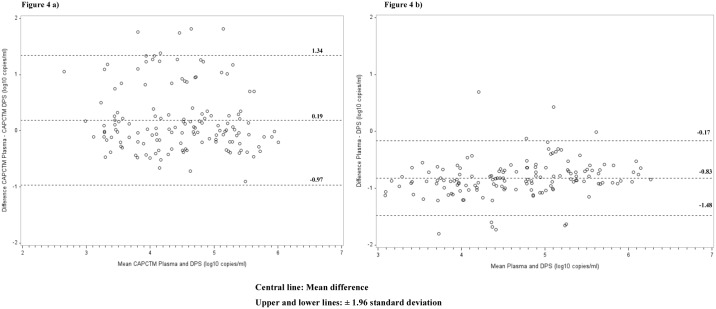
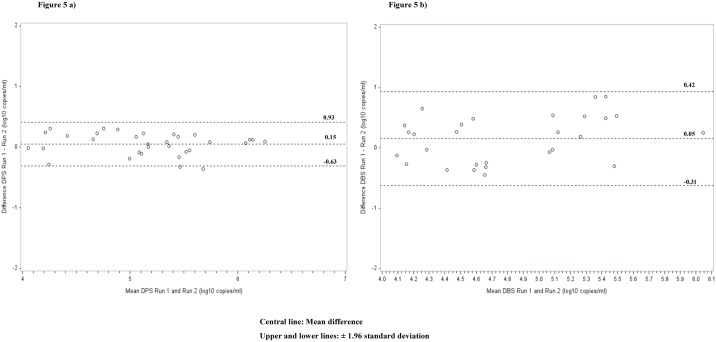
Using the Abbott test, the sensitivity and specificity, respectively, for DPS were (97.3%, [95%CI: 93.2-99.2] and 98.1% [95%CI: 89.7-100]) and those for DBS (93.9% [95%CI: 88.8-97.2] and 88.0% [95%CI: 82.2-92.4]). The correlation and agreement using paired plasma and DPS/DBS were strong, with r2 = 90.5 and rc = 68.1. The Bland-Altman relative percent change was 95.3 for DPS, (95%CI: 90.4-97.7) and 73.6 (95%CI: 51.6-86.5) for DBS. Using the CAP/CTM assay, the sensitivity for DBS was significantly higher compared to DPS (100.0% [95% CI: 97.6-100.0] vs. 94.7% [95%CI: 89.8-97.7]), while the specificity for DBS was lower: 4%, [95% CI: 0.4-13.7] compared to DPS: 94.0%, [95% CI: 83.5-98.7]. When compared under different clinical relevant thresholds, the accuracy for the Abbott assay was 95% at the 1000cps/ml cut-off with a sensitivity and specificity of 96.6% [95% CI 91.8-98.7] and 90.4% [95% CI 78.2-96.4] respectively. The optimum threshold was at 3000 cps/ml with an accuracy of 95.5%, sensitivity and specificity of 94.6% [95%CI 89.3-97.5] and 98.1% [95%CI 88.4-99.9]) respectively. The best threshold for CAP/CTM was at 4000 copies /mL, with 92.5% accuracy (sensitivity of 96.0% [95%CI 91.0-98.3] and specificity of 82.7% [95%CI 69.2-91.3]).
There was similar performance between matched DBS, DPS and plasma using the Abbott test, and good correlation for matched DPS and plasma using the CAPCTM test. The findings suggest that DBS and DPS may be reliably used as alternative specimens to plasma to measure HIV-1 VL using Abbott, and DPS may be reliably used with CAP/CTM in resource-limited settings.
在包括肯尼亚在内的大多数资源有限的地区,常规艾滋病毒病毒载量检测尚不普及。为了增加病毒载量检测的可及性,需要考虑并评估干血斑(DBS)等替代样本类型,其克服了与血浆分离和冷链运输相关的后勤障碍。本研究在肯尼亚西部使用雅培M 2000(Abbott)和罗氏Cobas Ampliprep/Cobas TaqMan(CAP/CTM)定量病毒载量检测方法,对匹配的干血斑(DBS)和干血浆斑(DPS)与血浆进行了评估。
从肯尼亚西部患者支持中心的200名有抗逆转录病毒治疗(ART)经验的HIV-1感染患者中获取匹配的血浆DBS和DPS。使用SAS 9.2版本在检测下限(CAP/CTM为400拷贝数/毫升,Abbott为550拷贝数/毫升)评估标准定量检测性能参数及伴随的95%置信区间(CI)。进一步使用受试者工作特征曲线(ROC)评估具有最佳检测性能的病毒载量阈值(参考检测方法为CAP/CTM血浆)。
使用雅培检测法,DPS的敏感性和特异性分别为(97.3%,[95%CI:93.2 - 99.2])和98.1%[95%CI:89.7 - 100]),DBS的敏感性和特异性分别为(93.9%[95%CI:88.8 - 97.2])和88.0%[95%CI:82.2 - 92.4])。配对血浆与DPS/DBS之间的相关性和一致性很强,r2 = 90.5,rc = 68.1。DPS的布兰德 - 奥特曼相对百分比变化为95.3(95%CI:90.4 - 97.7),DBS为73.6(95%CI:51.6 - 86.5)。使用CAP/CTM检测法,DBS的敏感性显著高于DPS(100.0%[95% CI:97.6 - 100.0]对94.7%[95%CI:89.8 - 97.7]),而DBS的特异性较低:4%,[95% CI:0.4 - 13.7],DPS为:94.0%,[95% CI:83.5 - 98.7]。在不同临床相关阈值下比较时,雅培检测法在1000拷贝数/毫升截断值时的准确性为95%,敏感性和特异性分别为96.6%[95% CI 91.8 - 98.7]和90.4%[95% CI 78.2 - 96.4]。最佳阈值为3000拷贝数/毫升,准确性为95.5%,敏感性和特异性分别为94.6%[95%CI 89.3 - 97.5]和98.1%[95%CI 88.4 - 99.9])。CAP/CTM的最佳阈值为4000拷贝数/毫升,准确性为92.5%(敏感性为96.0%[95%CI 91.0 - 98.3],特异性为82.7%[95%CI 69.2 - 91.3])。
使用雅培检测法时,匹配的DBS、DPS和血浆之间表现相似,使用CAPCTM检测法时,匹配的DPS和血浆之间具有良好的相关性。研究结果表明,DBS和DPS可以可靠地用作血浆的替代标本,以使用雅培检测法测量HIV-1病毒载量,并且在资源有限的环境中,DPS可以与CAP/CTM可靠地一起使用。