University of the Witwatersrand, Faculty of Health Sciences, School of Pathology, Department of Molecular Medicine and Haematology, Johannesburg, South Africa
National Health Laboratory Service, Johannesburg, South Africa.
J Clin Microbiol. 2019 Mar 28;57(4). doi: 10.1128/JCM.01336-18. Print 2019 Apr.
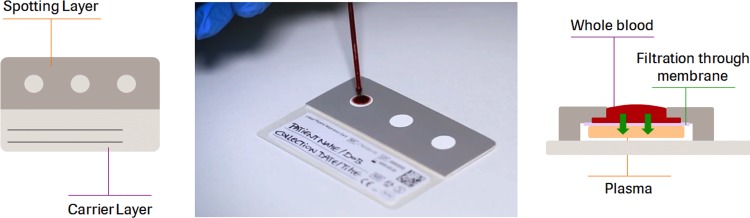
Plasma HIV viral load testing is the preferred means of monitoring antiretroviral treatment response. Dried blood spots (DBSs) hold considerable logistical advantages over EDTA samples, but they more frequently misclassify virological failure and have higher limits of detection (LoD). Plasma separation cards (PSCs) may overcome these limitations. Health workers collected EDTA whole blood by venipuncture and 140 μl of finger-prick blood by capillary tube from 53 HIV-infected adults. Capillary blood was immediately transferred to PSCs. Additionally, 432 EDTA samples from HIV-infected adults were spotted onto PSCs and analyzed together with the finger-prick samples. Specificity and sensitivity of PSC with paired EDTA-PSC samples tested on a cobas 6800/8800 system with the cobas HIV-1 test (cobas HIV) was determined. LoD (3rd HIV-1 WHO International Standard) and stability at a range of temperatures and storage durations was determined using cobas HIV and cobas AmpliPrep/cobas TaqMan HIV-1 test v2.0 (CAP/CTM). Of 132 specimens with quantitative values for paired EDTA-PSC samples, the mean log difference between samples was 0.05 copies/ml (95% confidence interval [CI], -0.01 to 0.11). The LoD for cobas HIV was 790.2 copies/ml and for CAP/CTM was 737.9 copies/ml. At 1,000 copies/ml, PSC sensitivity was 97.0% (128/132) and specificity was 97.2% (343/353). Results correlated well with those from EDTA samples (Deming = 0.90). PSC results were unaffected by temperature and storage conditions. PSC samples correlate well with plasma viral load and have adequate sensitivity and specificity. The improved performance may be as a result of a reduction in contribution from cell-associated viral nucleic acids. The card provides an alternative sample collection technology to DBSs.
血浆 HIV 病毒载量检测是监测抗逆转录病毒治疗反应的首选方法。干血斑 (DBS) 相对于 EDTA 样本具有相当大的后勤优势,但它们更频繁地错误分类病毒学失败,并且检测限 (LoD) 更高。血浆分离卡 (PSC) 可能克服这些限制。卫生工作者通过静脉穿刺采集 EDTA 全血,并用毛细管管从 53 名 HIV 感染成年人中采集 140μl 指尖血。毛细血管血立即转移到 PSC 上。此外,将 432 份来自 HIV 感染成年人的 EDTA 样本点样到 PSC 上,并与指尖血样本一起进行分析。使用 cobas 6800/8800 系统和 cobas HIV-1 测试 (cobas HIV) 对配对的 EDTA-PSC 样本进行检测,确定 PSC 的特异性和敏感性。使用 cobas HIV 和 cobas AmpliPrep/cobas TaqMan HIV-1 test v2.0 (CAP/CTM) 确定 3 级 HIV-1 WHO 国际标准的检测限 (LoD) 和在一系列温度和储存时间下的稳定性。在具有配对 EDTA-PSC 样本定量值的 132 份标本中,样本之间的平均对数差异为 0.05 拷贝/ml(95%置信区间 [CI],-0.01 至 0.11)。cobas HIV 的 LoD 为 790.2 拷贝/ml,CAP/CTM 的 LoD 为 737.9 拷贝/ml。在 1000 拷贝/ml 时,PSC 的灵敏度为 97.0%(128/132),特异性为 97.2%(343/353)。结果与 EDTA 样本的结果相关性良好(Deming = 0.90)。PSC 结果不受温度和储存条件的影响。PSC 样本与血浆病毒载量相关性良好,具有足够的灵敏度和特异性。性能的提高可能是由于细胞相关病毒核酸的贡献减少。该卡提供了一种替代 DBS 的样本采集技术。