Every-Palmer Susanna, Ellis Pete M
Te Korowai Whāriki Central Regional Forensic Service, Capital and Coast District Health Board, PO Box 50-233, Ratonga Rua-O-Porirua, Raiha Street, Porirua, Wellington, New Zealand.
Department of Psychological Medicine, University of Otago, Wellington, PO Box 7343, Wellington, 6242, New Zealand.
CNS Drugs. 2017 Aug;31(8):699-709. doi: 10.1007/s40263-017-0448-6.
Clozapine is the preferred antipsychotic for treatment-resistant schizophrenia, but has significant adverse effects, including gastrointestinal hypomotility or 'slow gut', which may result in severe constipation, ileus, bowel obstruction, and even death. These gastrointestinal effects remain inadequately recognized.
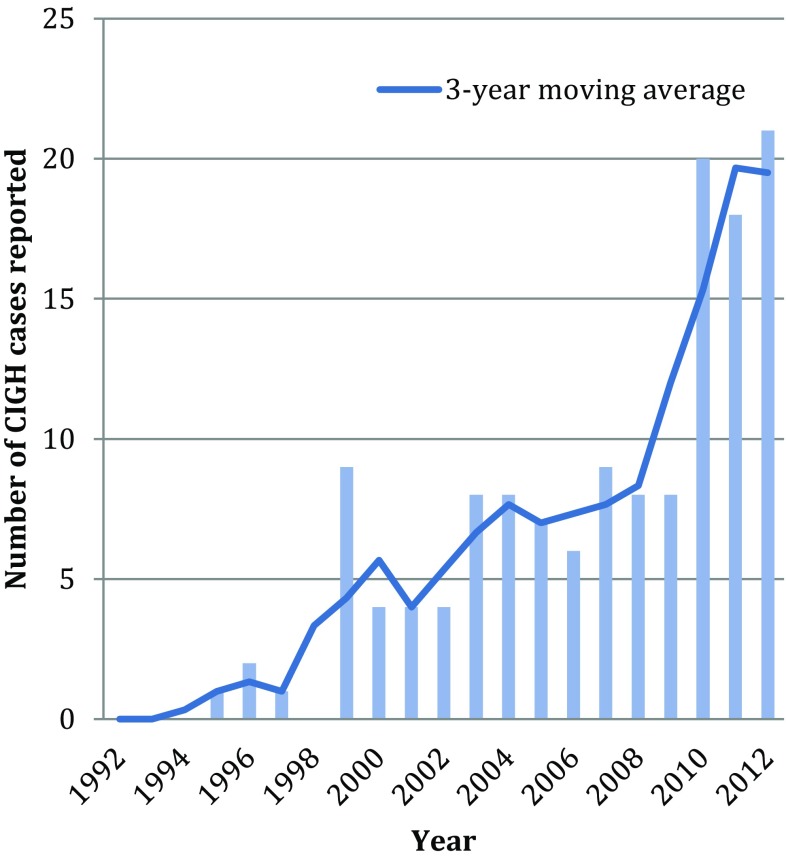
We reviewed all reports of serious clozapine-induced gastrointestinal hypomotility (CIGH) submitted to the Australian Therapeutic Goods Administration and New Zealand Pharmacovigilance Centre between 1992 and 2013. We extracted relevant demographic, clinical, and outcome data and derived a numerator from clozapine registries. We examined whether clozapine drug safety information in Australia, New Zealand, the US, and the UK was adequate and consistent with pharmacoepidemiologic evidence.
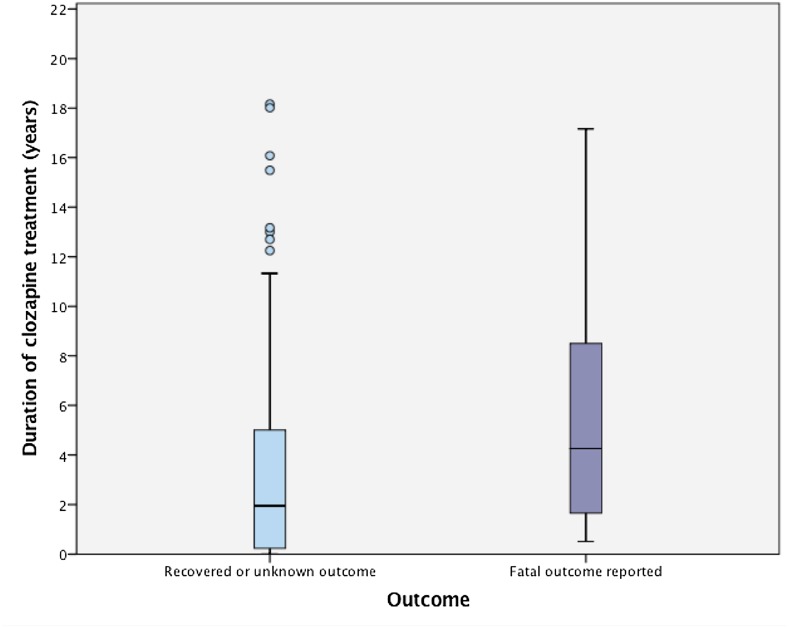
A total of 43,132 people commenced clozapine over the study period. 160 were reported as having serious gastrointestinal hypomotility with clozapine the suspected cause (37/10,000 clozapine users). Of these, 66.3% were male, age range was 17-76 years, clozapine dose range 25-1000 mg/day (mean 439 mg/day) and median duration of clozapine treatment 2.5 years. Few had received laxatives. At least 29 patients died (7/10,000 clozapine users), a reported case fatality rate of 18%. The CIGH prevalence, while similar to other smaller studies, differs significantly from clozapine prescribing information issued by regulators and pharmaceutical companies, none of which mention CIGH, and which report serious gastrointestinal complications at rates of <1/10,000, almost a 40-fold difference.
This is the largest study to date of serious CIGH. The reported prevalence of serious CIGH was 37/10,000, a likely underestimation of true prevalence. Current prescribing guidelines provide inadequate information on CIGH. This may be contributing to poor awareness and high associated morbidity and mortality. It is time regulators and manufacturers update their guidance.
氯氮平是治疗难治性精神分裂症的首选抗精神病药物,但具有显著的不良反应,包括胃肠道动力不足或“肠道蠕动缓慢”,这可能导致严重便秘、肠梗阻、肠阻塞,甚至死亡。这些胃肠道不良反应仍未得到充分认识。
我们回顾了1992年至2013年间提交给澳大利亚治疗用品管理局和新西兰药物警戒中心的所有关于氯氮平引起严重胃肠道动力不足(CIGH)的报告。我们提取了相关的人口统计学、临床和结局数据,并从氯氮平登记处得出分子数据。我们研究了澳大利亚、新西兰、美国和英国的氯氮平药物安全信息是否充分以及是否与药物流行病学证据一致。
在研究期间,共有43132人开始使用氯氮平。有160人被报告出现严重胃肠道动力不足,怀疑是氯氮平所致(每10000名氯氮平使用者中有37人)。其中,66.3%为男性,年龄范围为17至76岁,氯氮平剂量范围为25至1000毫克/天(平均439毫克/天),氯氮平治疗的中位持续时间为2.5年。很少有人使用过泻药。至少29名患者死亡(每10000名氯氮平使用者中有7人),报告的病死率为18%。CIGH的患病率虽然与其他较小规模的研究相似,但与监管机构和制药公司发布的氯氮平处方信息有显著差异,这些信息均未提及CIGH,且报告的严重胃肠道并发症发生率<1/10000,相差近40倍。
这是迄今为止关于严重CIGH的最大规模研究。报告的严重CIGH患病率为37/10000,可能低估了实际患病率。当前的处方指南关于CIGH的信息不足。这可能导致认识不足以及高相关发病率和死亡率。现在是监管机构和制造商更新其指南的时候了。