Murtaza Ghulam, Rahman Zia Ur, Sitwala Puja, Ladia Vatsal, Barad Bhavesh, Albalbissi Kais, Paul Timir K, Ramu Vijay
Department of Internal Medicine, East Tennessee State University, Johnson City, TN, USA.
Division of Cardiology, East Tennessee State University, Johnson City, TN, USA.
Clin Pract. 2017 Jun 7;7(3):950. doi: 10.4081/cp.2017.950.
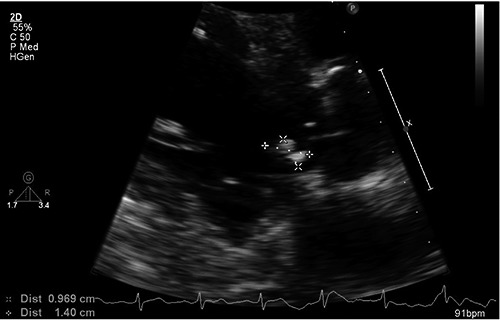
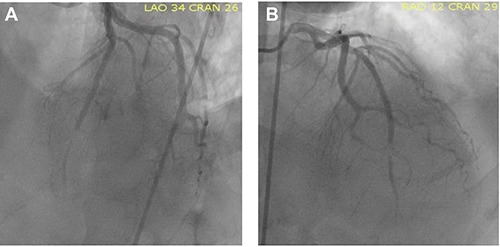
Embolic events from infective endocarditis can cause acute coronary syndrome. Mortality rate is high and optimal management might be different from those chosen in setting of classic atherosclerotic coronary artery disease. We present a case of 56-year-old male who had received 5 weeks of antibiotics for aortic valve endocarditis and developed acute ST segment elevation myocardial infarction in hospital settings. Interestingly, patient had recent left heart catheterization that was normal. This was recognized as embolic event from sterile vegetation. Patient was managed with balloon angioplasty and placement of intracoronary stent. Following re-vascularization, patient chest pain and electrocardiogram normalized and he improved in short term. However due to multiple comorbidities he had to be intubated and placed on dialysis.
感染性心内膜炎引发的栓塞事件可导致急性冠状动脉综合征。死亡率很高,其最佳治疗方案可能与经典动脉粥样硬化性冠状动脉疾病的治疗方案有所不同。我们报告一例56岁男性患者,该患者因主动脉瓣心内膜炎接受了5周抗生素治疗,并在住院期间发生急性ST段抬高型心肌梗死。有趣的是,患者近期的左心导管检查结果正常。这被认为是无菌赘生物引起的栓塞事件。患者接受了球囊血管成形术并植入了冠状动脉支架。血管重建后,患者胸痛症状和心电图恢复正常,短期内病情有所改善。然而,由于多种合并症,他不得不接受插管并进行透析治疗。