Baker David, Herrod Samuel S, Alvarez-Gonzalez Cesar, Zalewski Lukasz, Albor Christo, Schmierer Klaus
BartsMS (D.B., S.S.H., C.A.G., C.A., K.S.), Blizard Institute, ITS Research (L.Z.), Queen Mary University of London; and Barts Health NHS Trust (K.S.), Emergency Care & Acute Medicine Neuroscience Clinical Academic Group, London, UK.
Neurol Neuroimmunol Neuroinflamm. 2017 Jun 5;4(4):e360. doi: 10.1212/NXI.0000000000000360. eCollection 2017 Jul.
To understand the efficacy of cladribine (CLAD) treatment in MS through analysis of lymphocyte subsets collected, but not reported, in the pivotal phase III trials of cladribine and alemtuzumab induction therapies.
The regulatory submissions of the CLAD Tablets Treating Multiple Sclerosis Orally (CLARITY) (NCT00213135) cladribine and Comparison of Alemtuzumab and Rebif Efficacy in Multiple Sclerosis, study one (CARE-MS I) (NCT00530348) alemtuzumab trials were obtained from the European Medicine Agency through Freedom of Information requests. Data were extracted and statistically analyzed.
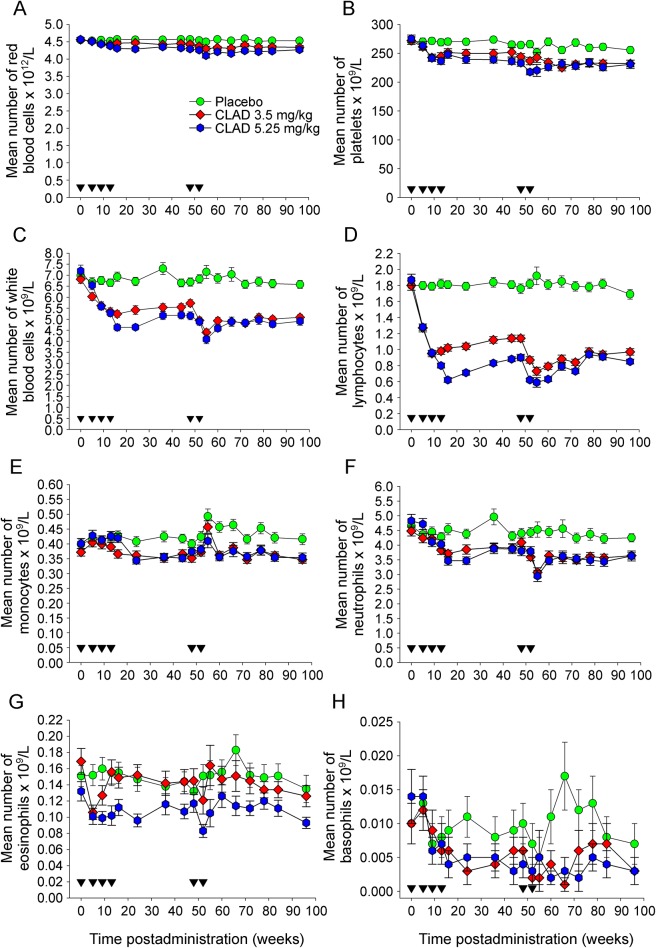
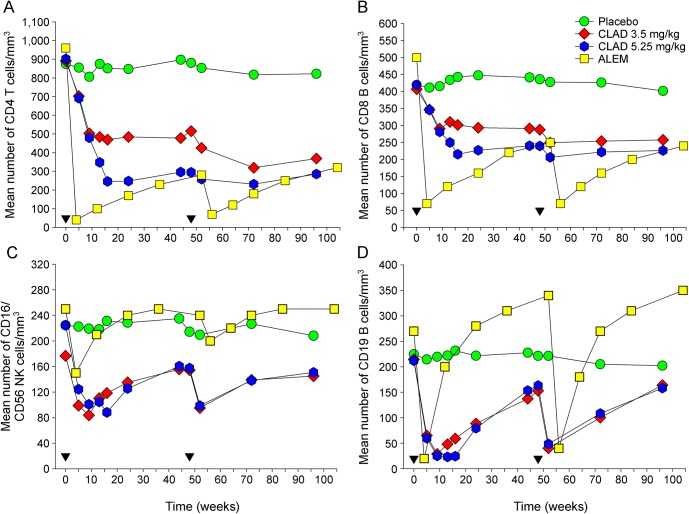
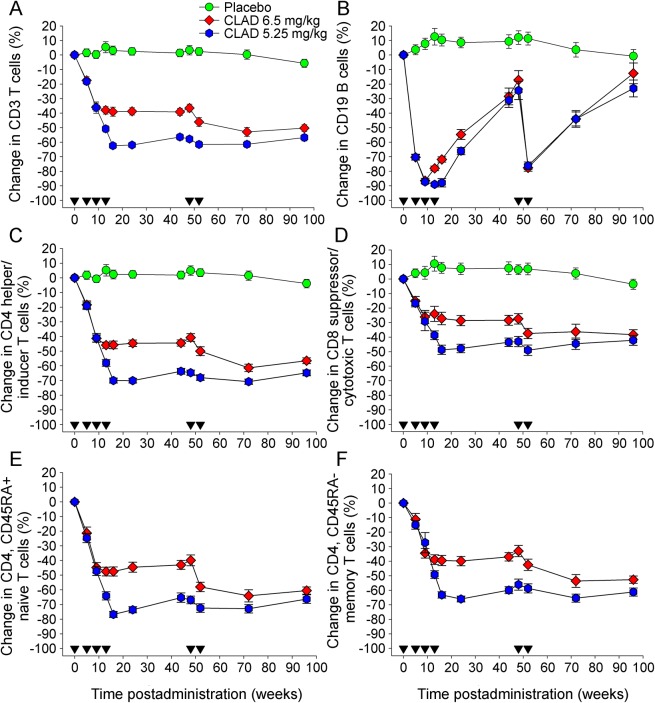
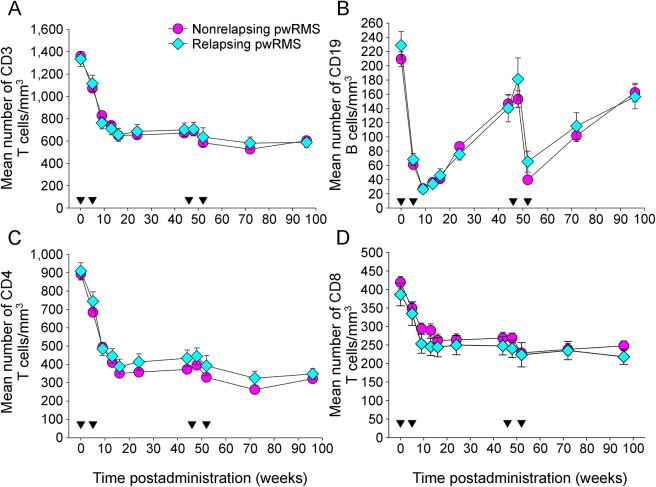
Either dose of cladribine (3.5 mg/kg; 5.25 mg/kg) tested in CLARITY reduced the annualized relapse rate to 0.16-0.18 over 96 weeks, and both doses were similarly effective in reducing the risk of MRI lesions and disability. Surprisingly, however, T-cell depletion was rather modest. Cladribine 3.5 mg/kg depleted CD4 cells by 40%-45% and CD8 cells by 15%-30%, whereas alemtuzumab suppressed CD4 cells by 70%-95% and CD8 cells by 47%-55%. However, either dose of cladribine induced 70%-90% CD19 B-cell depletion, similar to alemtuzumab (90%). CD19 cells slowly repopulated to 15%-25% of baseline before cladribine redosing. However, alemtuzumab induced hyperrepopulation of CD19 B cells 6-12 months after infusion, which probably forms the substrate for B-cell autoimmunities associated with alemtuzumab.
Cladribine induced only modest depletion of T cells, which may not be consistent with a marked influence on MS, based on previous CD4 T-cell depletion studies. The therapeutic drug-response relationship with cladribine is more consistent with lasting B-cell depletion and, coupled with the success seen with monoclonal CD20 depletion, suggests that B-cell suppression could be the major direct mechanism of action.
通过分析在克拉屈滨和阿仑单抗诱导治疗的关键III期试验中收集但未报告的淋巴细胞亚群,了解克拉屈滨(CLAD)治疗多发性硬化症(MS)的疗效。
通过信息公开申请从欧洲药品管理局获取口服克拉屈滨片治疗多发性硬化症(CLARITY)(NCT00213135)试验以及阿仑单抗与利比治疗多发性硬化症疗效比较研究一(CARE-MS I)(NCT00530348)试验的监管申报资料。提取数据并进行统计分析。
CLARITY试验中测试的任一剂量克拉屈滨(3.5 mg/kg;5.25 mg/kg)在96周内将年化复发率降至0.16 - 0.18,且两种剂量在降低MRI病灶风险和残疾风险方面同样有效。然而,令人惊讶的是,T细胞耗竭相当轻微。3.5 mg/kg克拉屈滨使CD4细胞减少40% - 45%,CD8细胞减少15% - 30%,而阿仑单抗使CD4细胞减少70% - 95%,CD8细胞减少47% - 55%。然而,任一剂量的克拉屈滨均可诱导70% - 90%的CD19 B细胞耗竭,与阿仑单抗(90%)相似。在重新给予克拉屈滨之前,CD19细胞缓慢恢复至基线的15% - 25%。然而,阿仑单抗在输注后6 - 12个月诱导CD19 B细胞过度增殖,这可能是与阿仑单抗相关的B细胞自身免疫的基础。
基于先前的CD4 T细胞耗竭研究,克拉屈滨仅引起适度的T细胞耗竭,这可能与对MS的显著影响不一致。克拉屈滨的治疗药物反应关系与持续的B细胞耗竭更为一致,并且与单克隆CD20耗竭的成功相结合,表明B细胞抑制可能是主要的直接作用机制。