Li Xi, Xu Zhiheng, Pang Xiaoqing, Huang Yongbo, Yang Baoxin, Yang Yuanyuan, Chen Kangxie, Liu Xiaoqing, Mao Pu, Li Yimin
State Key Laboratory of Respiratory Disease, Guangzhou Medical University, Guangzhou, Guangdong, China.
Intensive Care Unit, The People's Hospital Of Leshan, Sichuan, China.
PLoS One. 2017 Jun 19;12(6):e0179050. doi: 10.1371/journal.pone.0179050. eCollection 2017.
Immunosuppression is common even in the early stage of severe sepsis. Interleukin-10 (IL-10) secretion and lymphocyte exhaustion are the main features of sepsis-induced immunosuppression. However, the relationship between IL-10 and the lymphocyte is still unclear. We investigated if IL-10/lymphocyte ratio (IL10LCR) were associated with mortality in severe septic patients.
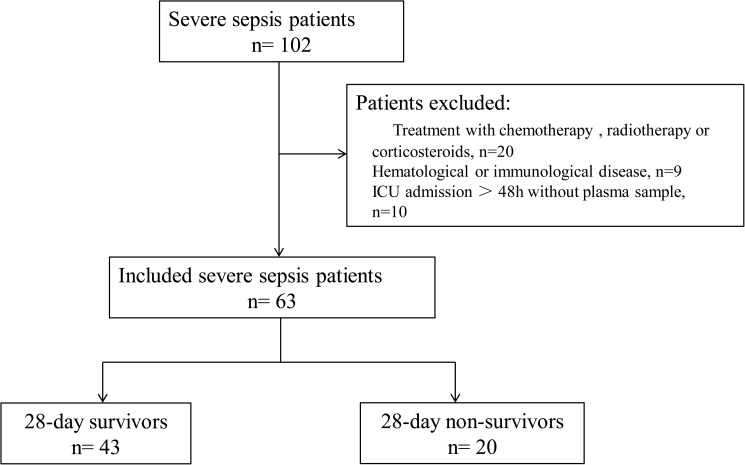
Adult patients with severe sepsis admitted to ICU of the First Affiliated Hospital of Guangzhou Medical University were identified from October 2012 to August 2013. Within 24 hours of ICU admission, peripheral whole blood was collected for the measurement of IL-10 using commercial multiplex bead-based assay kits and determination of lymphocyte count from laboratory data. The primary outcome was 28-day mortality.
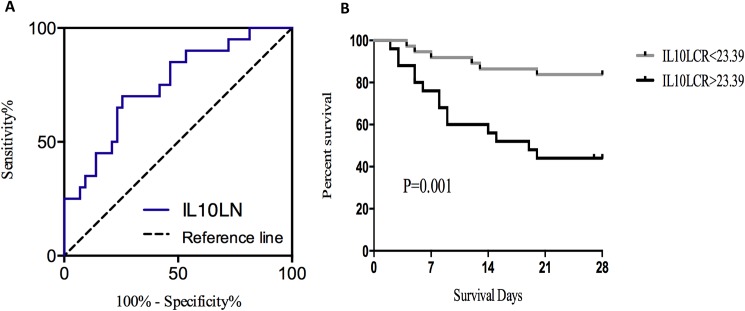
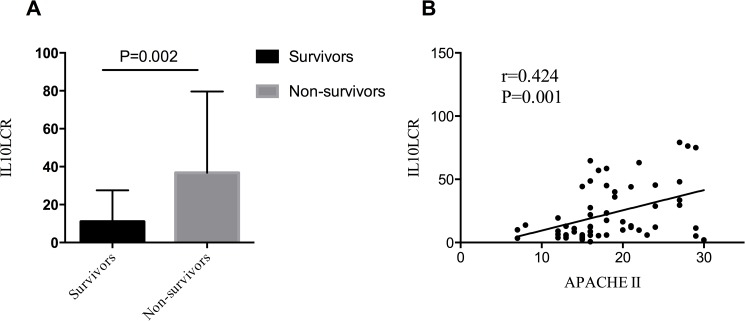
A total of 63 severe sepsis patients were identified. There were 20 (32%) patients died within 28 days. IL10LCR in non-survival patients was significantly higher than survival patients (median (IQR) 36.78 (12.34-79.63) ng/ml2 versus 11.01(5.41-27.50) ng/ml2, P = 0.002). Correlation analysis showed that IL10LCR was significantly correlated with APACHE II score (Spearman's rho = 0.424, P<0.001). The receiver operating characteristic (ROC) curves showed the area under the curve was 0.749 for IL10LCR level to predict 28-day mortality with sensitivity and specificity at 70.0% and 74.4%, respectively. At an optimal cutoff of 23.39ng/ml2, Kaplan-Meier curve showed survival in patients with IL10LCR level above 23.39ng/ml2 was significantly lower than in patients with IL10LCR level less than 23.39ng/ml2 (P = 0.001 by log-rank test).
IL10LCR level is significantly associated with the severity and outcome of severe septic patients. It may serve as a biomarker for sepsis-induced immunosuppression.
免疫抑制在严重脓毒症早期阶段就很常见。白细胞介素-10(IL-10)分泌和淋巴细胞耗竭是脓毒症诱导的免疫抑制的主要特征。然而,IL-10与淋巴细胞之间的关系仍不清楚。我们研究了IL-10/淋巴细胞比值(IL10LCR)是否与严重脓毒症患者的死亡率相关。
2012年10月至2013年8月期间,纳入广州医科大学附属第一医院重症监护病房收治的成年严重脓毒症患者。在入住重症监护病房24小时内,采集外周全血,使用基于多重微珠的商业检测试剂盒测定IL-10,并从实验室数据中确定淋巴细胞计数。主要结局为28天死亡率。
共纳入63例严重脓毒症患者。其中20例(32%)患者在28天内死亡。非存活患者的IL10LCR显著高于存活患者(中位数(四分位间距)36.78(12.34 - 79.63)ng/ml² 对 11.01(5.41 - 27.50)ng/ml²,P = 0.002)。相关性分析显示,IL10LCR与急性生理与慢性健康状况评分系统II(APACHE II)评分显著相关(斯皮尔曼等级相关系数 = 0.424,P < 0.001)。受试者工作特征(ROC)曲线显示,IL10LCR水平预测28天死亡率的曲线下面积为0.749,敏感性和特异性分别为70.0%和74.4%。在最佳截断值为23.39ng/ml²时,Kaplan-Meier曲线显示,IL10LCR水平高于23.39ng/ml²的患者生存率显著低于IL10LCR水平低于23.39ng/ml²的患者(对数秩检验,P = 0.001)。
IL10LCR水平与严重脓毒症患者的严重程度和结局显著相关。它可能作为脓毒症诱导的免疫抑制的生物标志物。