Brain Barriers Research Center, Department of Pharmaceutics, University of Minnesota, Minneapolis, MN, USA.
Radiation Oncology, Mayo Clinic, Rochester, MN, USA.
Pharmacol Res. 2017 Sep;123:10-25. doi: 10.1016/j.phrs.2017.06.008. Epub 2017 Jun 17.
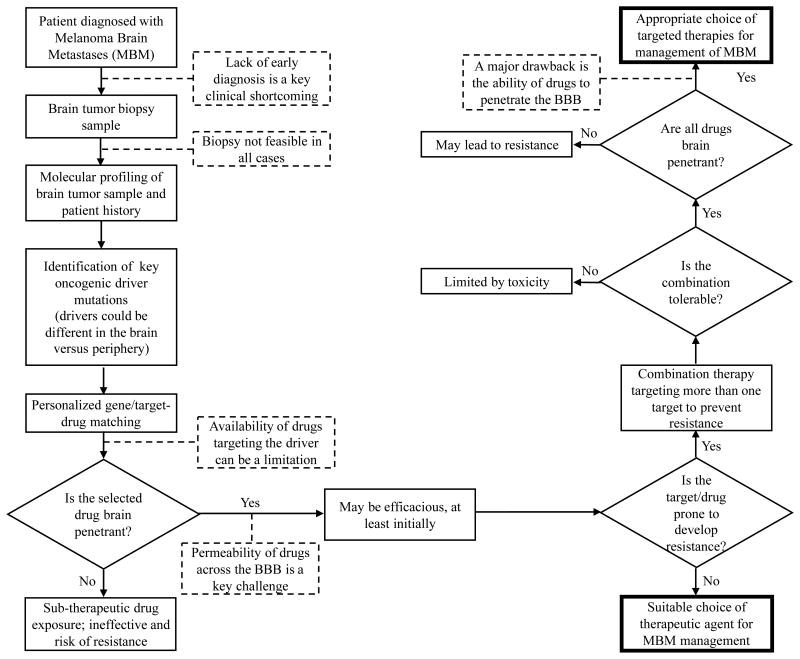
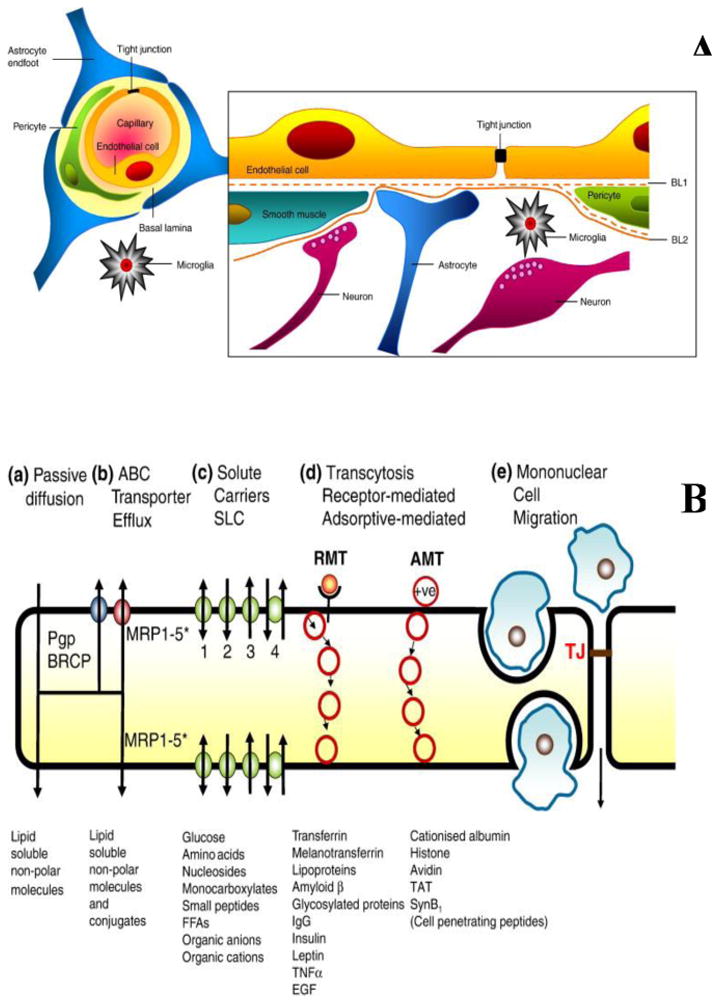
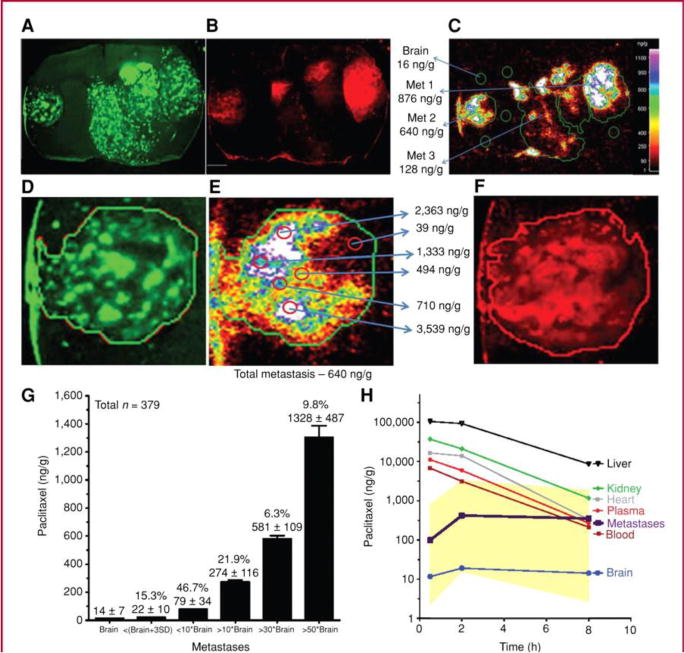
Melanoma has a high propensity to metastasize to the brain, and patients with melanoma brain metastases (MBM) have an extremely poor prognosis. The recent approval of several molecularly-targeted agents (e.g., BRAF, MEK inhibitors) and biologics (anti-CTLA-4, anti-PD-1 and anti-PD-L1 antibodies) has brought new hope to patients suffering from this formerly untreatable and lethal disease. Importantly, there have been recent reports of success in some clinical studies examining the efficacy of both targeted agents and immunotherapies that show similar response rates in both brain metastases and extracranial disease. While these studies are encouraging, there remains significant room for improvement in the treatment of MBM, given the lack of durable response and the development of resistance to current therapies. Critical questions remain regarding mechanisms that lead to this lack of durable response and development of resistance, and how those mechanisms may differ in systemic sites versus brain metastases. One issue that may not be fully appreciated is that the delivery of several small molecule molecularly-targeted therapies to the brain is often restricted due to active efflux at the blood-brain barrier (BBB) interface. Inadequate local drug concentrations may be partially responsible for the development of unique patterns of resistance at metastatic sites in the brain. It is clear that there can be local, heterogeneous BBB breakdown in MBM, as exemplified by contrast-enhancement on T1-weighted MR imaging. However, it is possible that the successful treatment of MBM with small molecule targeted therapies will depend, in part, on the ability of these therapies to penetrate an intact BBB and reach the protected micro-metastases (so called "sub-clinical" disease) that escape early detection by contrast-enhanced MRI, as well as regions of tumor within MRI-detectable metastases that may have a less compromised BBB. The emergence of resistance in MBM may be related to several diverse, yet interrelated, factors including the distinct microenvironment of the brain and inadequate brain penetration of targeted therapies to specific regions of tumor. The tumor microenvironment has been ascribed to play a key role in steering the course of disease progression, by dictating changes in expression of tumor drivers and resistance-related signaling mechanisms. Therefore, a key issue to consider is how changes in drug delivery, and hence local drug concentrations within a metastatic microenvironment, will influence the development of resistance. Herein we discuss our perspective on several critical questions that focus on many aspects relevant to the treatment of melanoma brain metastases; the answers to which may lead to important advances in the treatment of this devastating disease.
黑色素瘤有很高的向脑部转移的倾向,患有黑色素瘤脑转移(MBM)的患者预后极差。最近批准的几种分子靶向药物(例如 BRAF、MEK 抑制剂)和生物制剂(抗 CTLA-4、抗 PD-1 和抗 PD-L1 抗体)为这种以前无法治疗和致命的疾病患者带来了新的希望。重要的是,最近有一些临床研究报告成功地检测了靶向药物和免疫疗法的疗效,这些研究在脑转移和颅外疾病中显示出相似的反应率。尽管这些研究令人鼓舞,但鉴于目前治疗方法缺乏持久反应和耐药性的发展,MBM 的治疗仍有很大的改进空间。对于导致这种缺乏持久反应和耐药性发展的机制,以及这些机制在系统部位与脑转移部位之间可能有何不同,仍存在许多关键问题。一个可能尚未充分认识到的问题是,由于血脑屏障(BBB)界面的主动外排,几种小分子分子靶向疗法向脑部的输送往往受到限制。局部药物浓度不足可能是导致脑转移部位出现独特耐药模式的部分原因。显然,MBM 中可能存在局部、异质的 BBB 破裂,如 T1 加权磁共振成像上的对比增强所示。然而,用小分子靶向疗法成功治疗 MBM,可能部分取决于这些疗法穿透完整的 BBB 并到达通过对比增强 MRI 早期检测到的保护性微转移(所谓的“亚临床”疾病)的能力,以及 MRI 可检测到的转移瘤内可能 BBB 受损较少的区域。MBM 中的耐药性的出现可能与几种不同但相互关联的因素有关,包括大脑的独特微环境和靶向治疗对肿瘤特定区域的脑穿透不足。肿瘤微环境被认为在决定肿瘤驱动因素和耐药相关信号机制的表达变化方面起着关键作用,从而影响疾病进展的过程。因此,一个关键问题是考虑药物输送的变化,以及转移瘤微环境中局部药物浓度的变化,将如何影响耐药性的发展。本文我们讨论了我们对几个关键问题的看法,这些问题集中在与黑色素瘤脑转移治疗相关的许多方面;这些问题的答案可能会推动这种毁灭性疾病治疗的重要进展。