Baron Frédéric, Ruggeri Annalisa, Beohou Eric, Labopin Myriam, Mohty Mohamad, Blaise Didier, Cornelissen Jan J, Chevallier Patrice, Sanz Guillermo, Petersen Eefke, Savani Bipin N, Gluckman Eliane, Nagler Arnon
Department of Hematology, University of Liege, CHU Sart-Tilman, 4000, Liege, Belgium.
Eurocord, Hospital Saint Louis, AP-HP, and IUH University Paris VII, Paris, France.
J Hematol Oncol. 2017 Jun 21;10(1):128. doi: 10.1186/s13045-017-0497-9.
The feasibility of cord blood transplantation (CBT) in adults is limited by the relatively low number of hematopoietic stem/progenitor cells contained in one single CB unit. The infusion of two CB units from different partially HLA-matched donors (double CBT) is frequently performed in patients who lack a sufficiently rich single CB unit.
We compared CBT outcomes in patients given single or double CBT following reduced-intensity conditioning (RIC) in a retrospective multicenter registry-based study. Inclusion criteria included adult (≥18 years) patients, acute myeloid leukemia (AML) or acute lymphoblastic leukemia (ALL), complete remission (CR) at the time of transplantation, first single (with a cryopreserved TNC ≥ 2.5 × 10/kg) or double CBT between 2004 and 2014, and RIC conditioning.
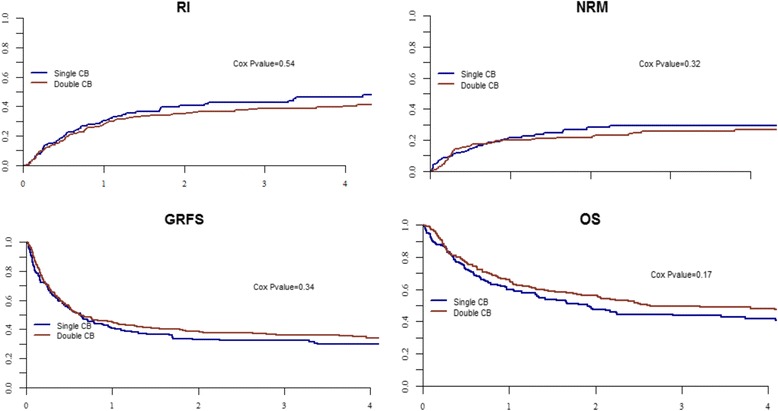
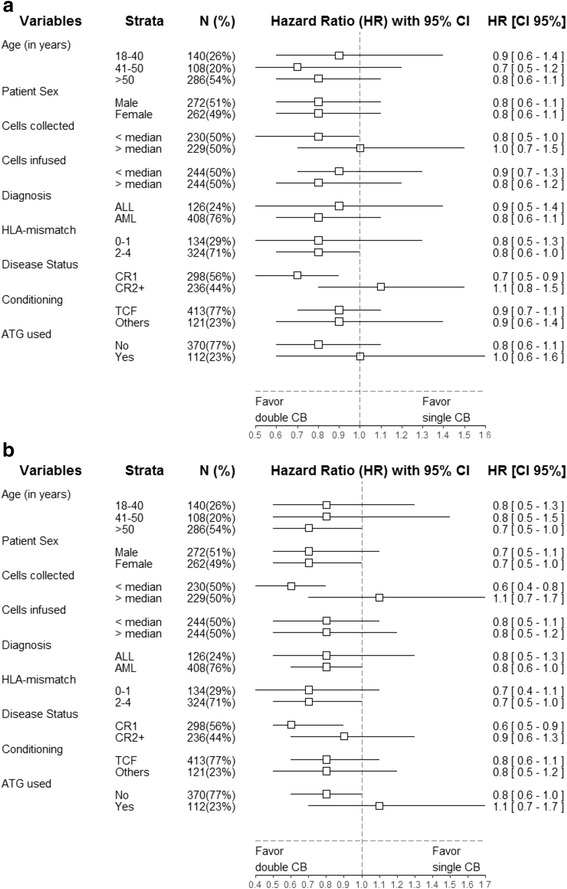
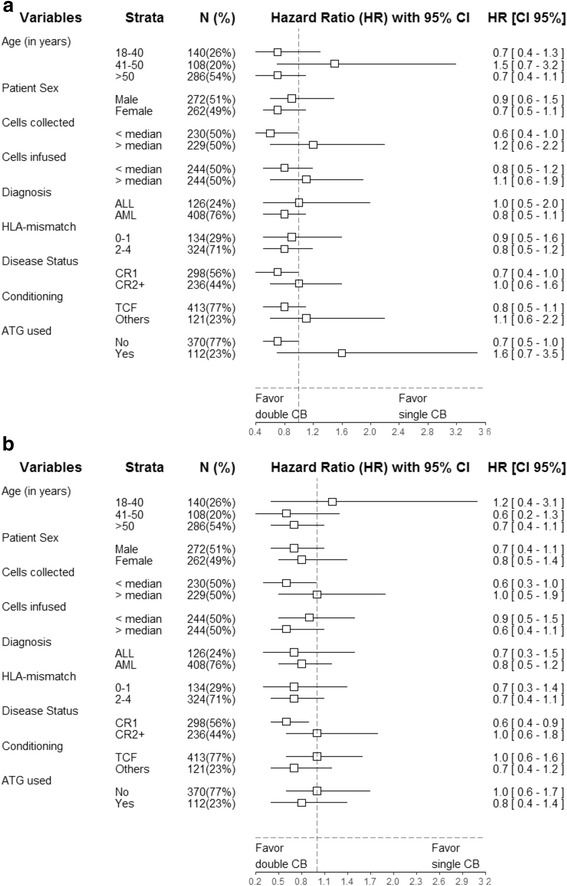
Data from 534 patients with AML (n = 408) or ALL (n = 126) receiving a first single (n = 172) or double (n = 362) CBT were included in the analyses. In univariate analysis, in comparison to patients transplanted with a single CB, double CB recipients had a similar incidence of neutrophil engraftment but a suggestion for a higher incidence of grade II-IV acute GVHD (36 versus 28%, P = 0.08). In multivariate analyses, in comparison to single CBT recipients, double CBT patients had a comparable incidence of relapse (HR = 0.9, P = 0.5) and of nonrelapse mortality (HR = 0.8, P = 0.3), as well as comparable overall (HR = 0.8, P = 0.17), leukemia-free (HR = 0.8, P = 0.2) and GVHD-free, relapse-free (HR = 1.0, P = 0.3) survival.
These data failed to demonstrate better transplantation outcomes in adult patients receiving double CBT in comparison to those receiving single CBT with adequate TNC after RIC.
成人脐血移植(CBT)的可行性受到单个脐血单位中造血干/祖细胞数量相对较少的限制。对于缺乏足够丰富的单个脐血单位的患者,经常会输注来自不同部分人类白细胞抗原(HLA)匹配供体的两个脐血单位(双份CBT)。
在一项基于多中心登记的回顾性研究中,我们比较了接受减低强度预处理(RIC)的单份或双份CBT患者的CBT结果。纳入标准包括成年(≥18岁)患者、急性髓系白血病(AML)或急性淋巴细胞白血病(ALL)、移植时处于完全缓解(CR)状态、2004年至2014年间首次进行单份(冷冻保存的总核细胞数[TNC]≥2.5×10⁸/kg)或双份CBT以及RIC预处理。
分析纳入了534例接受首次单份(n = 172)或双份(n = 362)CBT的AML(n = 408)或ALL(n = 126)患者的数据。在单因素分析中,与接受单份脐血移植的患者相比,接受双份脐血移植的患者中性粒细胞植入发生率相似,但提示II-IV级急性移植物抗宿主病(GVHD)发生率较高(36%对28%,P = 0.08)。在多因素分析中,与单份CBT受者相比,双份CBT患者的复发率(风险比[HR] = 0.9,P = 0.5)和非复发死亡率(HR = 0.8,P = 0.3)相当,总体生存率(HR = 0.8,P = 0.17)、无白血病生存率(HR = 0.8,P = 0.2)以及无GVHD、无复发生存率(HR = 1.0,P = 0.3)也相当。
这些数据未能证明与接受RIC后具有足够TNC的单份CBT的成年患者相比,接受双份CBT的成年患者具有更好的移植结果。