Goossens Nicolas, Singal Amit G, King Lindsay Y, Andersson Karin L, Fuchs Bryan C, Besa Cecilia, Taouli Bachir, Chung Raymond T, Hoshida Yujin
Division of Liver Diseases, Department of Medicine, Liver Cancer Program, Tisch Cancer Institute, Graduate School of Biomedical Sciences, Icahn School of Medicine at Mount Sinai, New York, New York, USA.
Division of Gastroenterology and Hepatology, Geneva University Hospital, Geneva, Switzerland.
Clin Transl Gastroenterol. 2017 Jun 22;8(6):e101. doi: 10.1038/ctg.2017.26.
Hepatocellular carcinoma (HCC) surveillance with biannual ultrasound is currently recommended for all patients with cirrhosis. However, clinical implementation of this "one-size-fits-all" approach is challenging as evidenced by its low application rate. We aimed to evaluate the cost-effectiveness of risk-stratified HCC surveillance strategies in patients with cirrhosis.
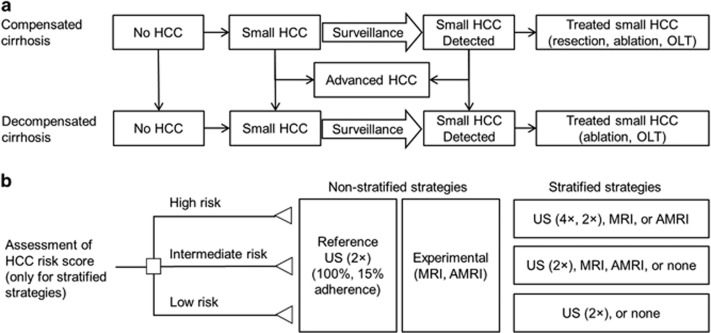
A Markov decision-analytic modeling was performed to simulate a cohort of 50-year-old subjects with compensated cirrhosis. Risk-stratified HCC surveillance strategies was implemented, in which patients were stratified into high-, intermediate-, or low-risk groups by HCC risk biomarker-based scores and assigned to surveillance modalities tailored to HCC risk (2 non-risk-stratified and 14 risk-stratified strategies) and compared with non-stratified biannual ultrasound.
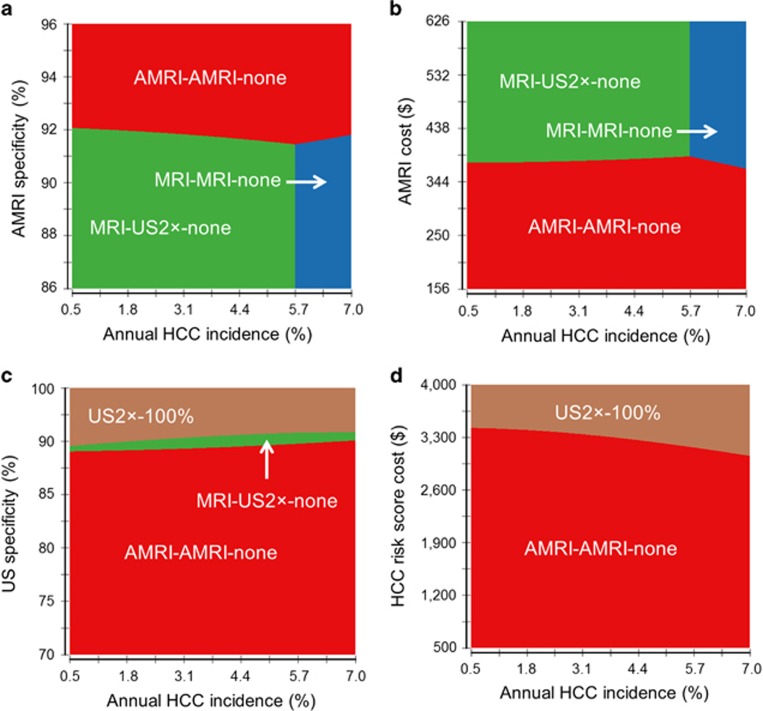
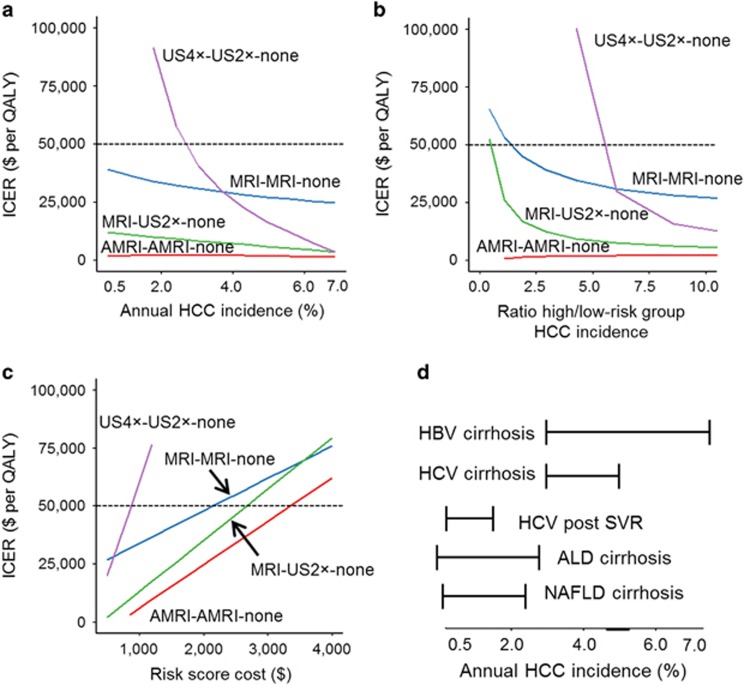
Quality-adjusted life expectancy gains for biannual ultrasound in all patients and risk-stratified strategies compared with no surveillance were 1.3 and 0.9-2.1 years, respectively. Compared with the current standard of biannual ultrasound in all cirrhosis patients, risk-stratified strategies applying magnetic resonance imaging (MRI) and/or ultrasound only in high- and intermediate-risk patients, without screening in low-risk patients, were cost-effective. Abbreviated MRI (AMRI) for high- and intermediate-risk patients had the lowest incremental cost-effectiveness ratio (ICER) of $2,100 per quality-adjusted life year gained. AMRI in intermediate- and high-risk patients had ICERs <$3,000 across a wide range of HCC incidences.
Risk-stratified HCC surveillance strategies targeting high- and intermediate-risk patients with cirrhosis are cost-effective and outperform the currently recommended non-stratified biannual ultrasound in all patients with cirrhosis.
目前建议对所有肝硬化患者每半年进行一次超声检查以监测肝细胞癌(HCC)。然而,这种“一刀切”方法的临床实施具有挑战性,其低应用率就证明了这一点。我们旨在评估肝硬化患者中风险分层的HCC监测策略的成本效益。
进行马尔可夫决策分析模型,以模拟一组50岁的代偿期肝硬化受试者。实施风险分层的HCC监测策略,根据基于HCC风险生物标志物的评分将患者分为高、中、低风险组,并根据HCC风险分配至相应的监测方式(2种非风险分层和14种风险分层策略),并与非分层的半年一次超声检查进行比较。
与不进行监测相比,所有患者半年一次超声检查以及风险分层策略的质量调整生命预期分别增加1.3年和0.9 - 2.1年。与目前所有肝硬化患者每半年进行一次超声检查的标准相比,仅对高风险和中风险患者应用磁共振成像(MRI)和/或超声检查、不对低风险患者进行筛查的风险分层策略具有成本效益。针对高风险和中风险患者的简化MRI(AMRI)每获得一个质量调整生命年的增量成本效益比(ICER)最低,为2100美元。在广泛的HCC发病率范围内,中高风险患者的AMRI的ICER < 3000美元。
针对肝硬化高风险和中风险患者的风险分层HCC监测策略具有成本效益,并且优于目前建议的所有肝硬化患者非分层半年一次超声检查。