Rohde Carmen, Thiele Alena Gerlinde, Och Ulrike, Schönherr Katrin, Meyer Uta, Rosenbaum-Fabian Stefanie, Maddalon Cornelia, Matzken Sabine, Blessing Holger, Lang Frauke, Jörg-Streller Monika, Beblo Skadi
Hospital for Children and Adolescents, Department of Women and Child Health, University Hospitals, University of Leipzig, Liebigstraße 20 a, 04103 Leipzig, Germany.
Muenster University Children's Hospital, Albert-Schweitzer-Campus 1, 48149 Münster, Germany.
Mol Genet Metab Rep. 2015 Oct 22;5:36-41. doi: 10.1016/j.ymgmr.2015.09.006. eCollection 2015 Dec.
A phenylalanine (Phe) restricted dietary management is required in phenylketonuria (PKU) to maintain good metabolic control. Nevertheless, five different models of dietary regimes, which differ in their accuracy of Phe documentation, are used. To investigate the effect of the dietary regime on metabolic control, a multicenter evaluation was performed.
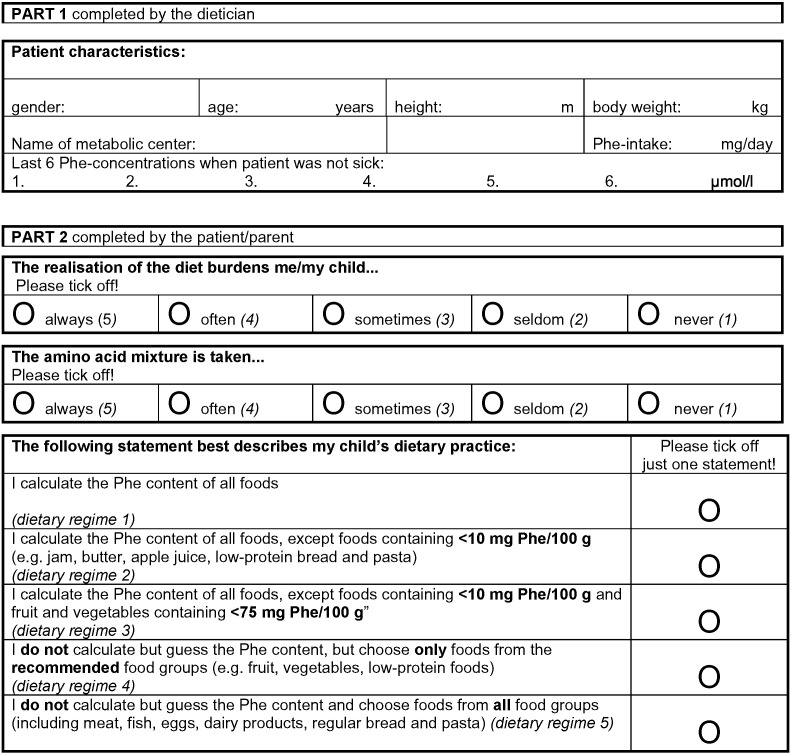
PATIENTS/METHODS: 149 patients (max. 800 mg Phe-intake/day; 108 children aged 1-9 years and 41 adolescents aged 10-15 years) could be included. They were separated according to age and dietary regime, revealed by a questionnaire on dietary habits. Dietary regimes vary from daily strict calculation of all Phe-intake (group 1) to a rather loose regime only estimating Phe-intake and including high protein food (group 5). Data were analyzed with respect to metabolic control (Phe-concentrations, Phe-concentrations above upper recommended limit during 6 months before the interview), Phe-intake (mg/day) and age (years).
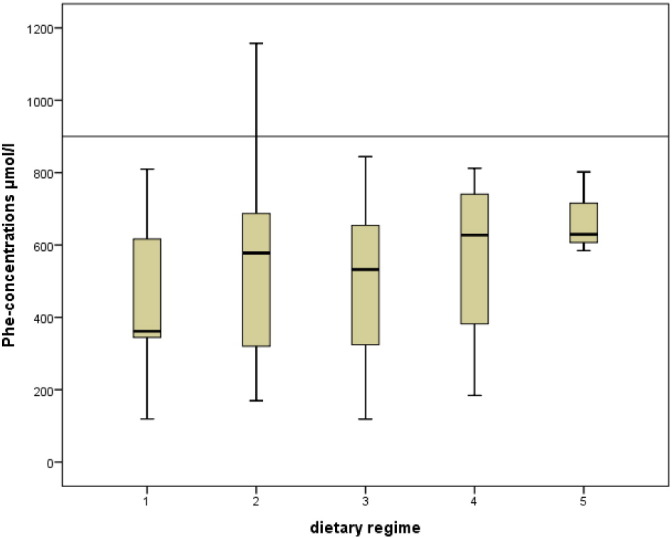
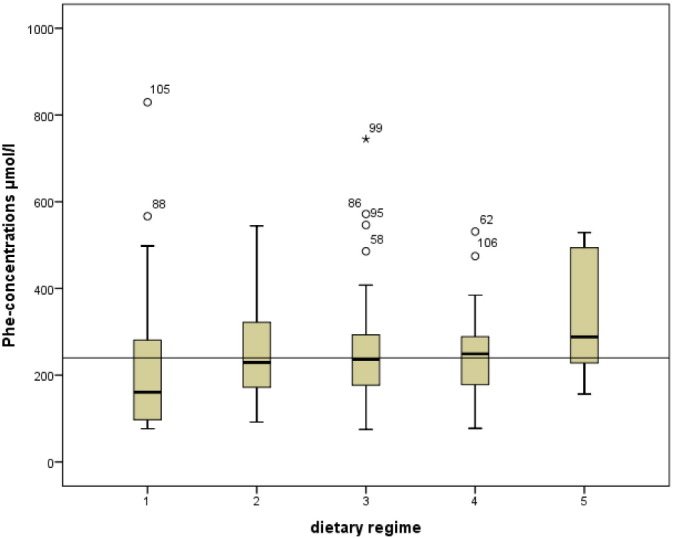
Median Phe-concentrations in children did not differ significantly among diet groups (group 1: 161; 2: 229, 3: 236, 4: 249, 5: 288 μmol/l, p = 0.175). However, exact daily Phe calculation led to significantly lower percentage of Phe concentrations above the upper recommended limit (group 1: 17, 2: 50, 3: 42, 4: 50, 5: 75%, p = 0.035). All included patients showed good to acceptable metabolic control. Patients on the dietary regime with the least accuracy, consuming also high protein foods, showed the poorest metabolic control. Median Phe concentrations of all other groups remained within recommended ranges, including from groups not calculating special low protein foods, fruit and vegetables and using a simplified system of recording Phe-intake. In adolescents no significant differences among diet groups were revealed.
Exact calculation of Phe content of all food is not necessary to achieve good metabolic control in children and adolescents with PKU. Excluding special low protein food, as well as fruit and vegetables from calculation of Phe-intake has no impact on metabolic control. However including protein rich food into the diet and simply estimating all Phe-intake appears insufficient. The simplification of dietary regime may be helpful in enhancing acceptability and feasibility.
苯丙酮尿症(PKU)患者需要进行苯丙氨酸(Phe)限制饮食管理以维持良好的代谢控制。然而,目前使用了五种不同的饮食方案模型,它们在Phe记录的准确性方面存在差异。为了研究饮食方案对代谢控制的影响,进行了一项多中心评估。
患者/方法:纳入了149例患者(最大Phe摄入量为每日800毫克;108名1至9岁儿童和41名10至15岁青少年)。根据年龄和饮食习惯问卷所显示的饮食方案对他们进行分组。饮食方案从严格每日计算所有Phe摄入量(第1组)到仅估算Phe摄入量并包括高蛋白食物的较为宽松的方案(第5组)不等。分析了有关代谢控制(Phe浓度、访谈前6个月内高于推荐上限的Phe浓度)、Phe摄入量(毫克/天)和年龄(岁)的数据。
各饮食组儿童的Phe浓度中位数无显著差异(第1组:161;第2组:229,第3组:236,第4组:249,第5组:288μmol/l,p = 0.175)。然而,精确计算每日Phe摄入量导致高于推荐上限的Phe浓度百分比显著降低(第1组:17%,第2组:50%,第3组:42%,第4组:50%,第5组:75%,p = 0.035)。所有纳入患者均表现出良好至可接受的代谢控制。饮食方案准确性最低且食用高蛋白食物的患者代谢控制最差。所有其他组的Phe浓度中位数均保持在推荐范围内,包括那些不计算特殊低蛋白食物、水果和蔬菜且使用简化Phe摄入量记录系统的组。青少年各饮食组之间未发现显著差异。
对于PKU儿童和青少年,要实现良好的代谢控制,无需精确计算所有食物的Phe含量。在计算Phe摄入量时排除特殊低蛋白食物以及水果和蔬菜对代谢控制没有影响。然而,将富含蛋白质的食物纳入饮食且仅简单估算所有Phe摄入量似乎是不够的。简化饮食方案可能有助于提高可接受性和可行性。