Jensen Majken Linnemann, Jørgensen Marit Eika, Hansen Ebba Holme, Aagaard Lise, Carstensen Bendix
Steno Diabetes Center Copenhagen, Gentofte, Denmark.
Faculty of Health and Medical Sciences, Department of Pharmacy, Section for Social and Clinical Pharmacy, Universitetsparken 2, University of Copenhagen, Denmark.
PLoS One. 2017 Jun 30;12(6):e0179546. doi: 10.1371/journal.pone.0179546. eCollection 2017.
Poor adherence to medication therapy among type 2 diabetes patients is a clinical challenge. We aimed to determine which factors are associated with the three phases of long-term adherence to medication: initiation, implementation and discontinuation in a register-based study.
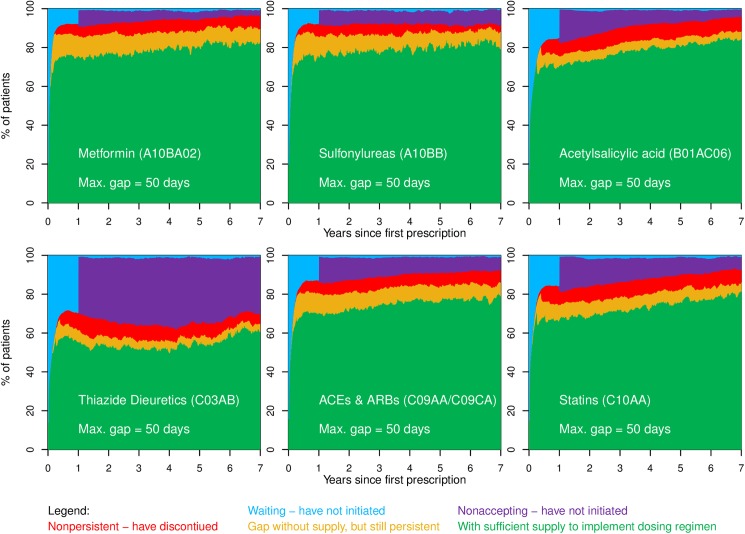
Adherence to six medicine groups (metformin, sulfonylureas, acetylsalicylic acid, thiazide diuretics, renin angiotensin system inhibitors, and statins) were analysed among 5,232 patients with type 2 diabetes at a tertiary referral hospital during 1998-2009. Rate-ratios of initiation of treatment, recurrent gaps in supply of medication, and discontinuation of treatment were analysed using Poisson regression.
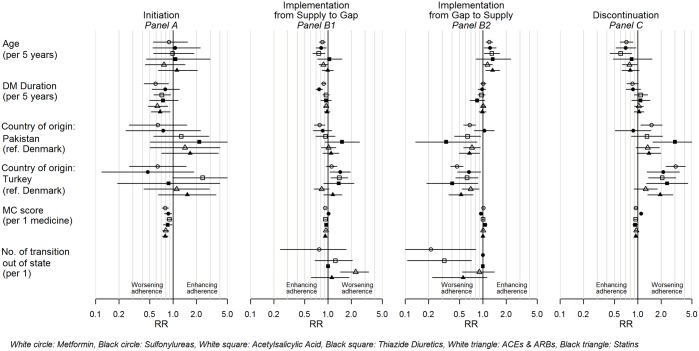
Poor initiation rather than poor implementation or discontinuation was the main contributor to medication nonadherence. Polypharmacy was a risk factor for slower initiation of treatment for all six medicine groups (rate ratio ranging 0.79 95%CI [0.72-0.87] to 0.89 95%CI [0.82-0.96] per already prescribed medicine), but once patients were in treatment, polypharmacy was not associated with recurrence of gaps in supply of medication, and polypharmacy was associated with lower risk of discontinuation (rate ratio ranging 0.93 95%CI [0.86-1.00] to 0.96 95%CI [0.93-0.99] per prescribed medicine). Other identified risk factors for slow initiation, poor implementation, and discontinuation were diabetes duration, younger age, and Turkish/Pakistani origin.
This study showed that a risk factor does not necessarily have the same association with all three elements of adherence (initiation, implementation and discontinuation), and that efforts supporting patients introduced to more complex drug combinations should be prioritized.
2型糖尿病患者药物治疗依从性差是一项临床挑战。我们旨在通过一项基于登记的研究确定哪些因素与长期药物治疗依从性的三个阶段(起始、实施和停药)相关。
对1998 - 2009年期间在一家三级转诊医院的5232例2型糖尿病患者使用的六类药物(二甲双胍、磺脲类、乙酰水杨酸、噻嗪类利尿剂、肾素血管紧张素系统抑制剂和他汀类药物)的依从性进行分析。使用泊松回归分析治疗起始率、药物供应反复中断率和治疗中断率。
药物治疗不依从的主要原因是起始不佳,而非实施或停药不佳。联合用药是所有六类药物治疗起始较慢的危险因素(每增加一种已处方药物,率比范围为0.79 95%置信区间[0.72 - 0.87]至0.89 95%置信区间[0.82 - 0.96]),但一旦患者开始治疗,联合用药与药物供应中断复发无关,且联合用药与停药风险较低相关(每增加一种已处方药物,率比范围为0.93 95%置信区间[0.86 - 1.00]至0.96 95%置信区间[0.93 - 0.99])。其他确定的起始慢、实施差和停药的危险因素包括糖尿病病程、年轻以及土耳其/巴基斯坦裔。
本研究表明,一个危险因素不一定与依从性的所有三个要素(起始、实施和停药)都有相同的关联,并且应优先努力支持开始使用更复杂药物组合的患者。