Phan Binh An P, Weigel Bernard, Ma Yifei, Scherzer Rebecca, Li Danny, Hur Sophia, Kalapus S C, Deeks Steven, Hsue Priscilla
From the Division of Cardiology, Department of Medicine (B.A.P.P., B.W., Y.M., D.L., S.H., S.C.K., P.H.), Positive Health Program (S.D.), San Francisco General Hospital, University of California; and Department of Medicine, San Francisco Veteran's Affairs Medical Center, University of California (R.S.).
Circ Cardiovasc Imaging. 2017 Jul;10(7):e005995. doi: 10.1161/CIRCIMAGING.116.005995.
Although HIV is associated with increased atherosclerotic cardiovascular disease (CVD) risk, it is unknown whether guidelines can identify HIV-infected adults who may benefit from statins. We compared the 2013 American College of Cardiology/American Heart Association and 2004 Adult Treatment Panel III recommendations in HIV-infected adults and evaluated associations with carotid artery intima-media thickness and plaque.
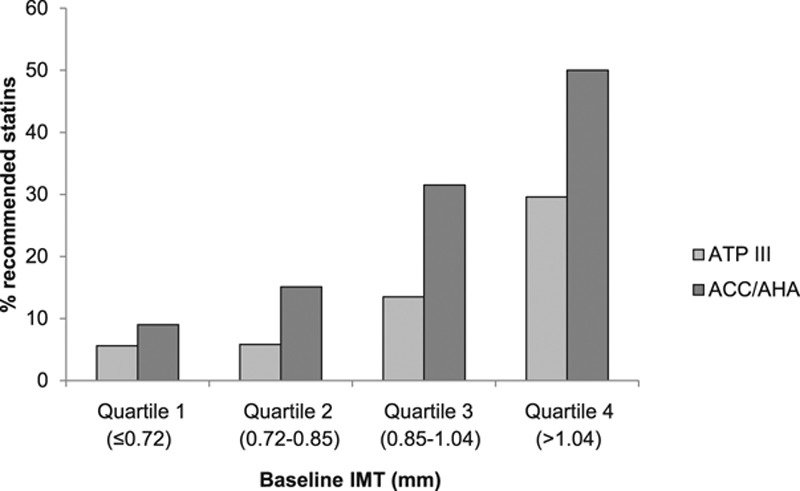
Carotid artery intima-media thickness was measured at baseline and 3 years later in 352 HIV-infected adults without clinical atherosclerotic CVD and not on statins. Plaque was defined as IMT >1.5 mm in any segment. At baseline, the median age was 43 (interquartile range, 39-49), 85% were men, 74% were on antiretroviral medication, and 50% had plaque. The American College of Cardiology/American Heart Association guidelines were more likely to recommend statins compared with the Adult Treatment Panel III guidelines, both overall (26% versus 14%; <0.001), in those with plaque (32% versus 17%; =0.0002), and in those without plaque (16% versus 7%; =0.025). In multivariable analysis, older age, higher low-density lipoprotein cholesterol, pack per year of smoking, and history of opportunistic infection were associated with baseline plaque. Baseline IMT (hazard ratio, 1.18 per 10% increment; 95% confidence interval, 1.05-1.33; =0.005) and plaque (hazard ratio, 2.06; 95% confidence interval, 1.02-4.08; =0.037) were each associated with all-cause mortality, independent of traditional CVD risk factors.
Although the American College of Cardiology/American Heart Association guidelines recommended statins to a greater number of HIV-infected adults compared with the Adult Treatment Panel III guidelines, both failed to recommend therapy in the majority of HIV-affected adults with carotid plaque. Baseline carotid atherosclerosis but not atherosclerotic CVD risk scores was an independent predictor of mortality. HIV-specific guidelines that include detection of subclinical atherosclerosis may help to identify HIV-infected adults who are at increased atherosclerotic CVD risk and may be considered for statins.
尽管HIV与动脉粥样硬化性心血管疾病(CVD)风险增加相关,但尚不清楚指南能否识别出可能从他汀类药物治疗中获益的HIV感染成人。我们比较了2013年美国心脏病学会/美国心脏协会与2004年成人治疗小组III针对HIV感染成人的推荐,并评估了与颈动脉内膜中层厚度及斑块的相关性。
对352例无临床动脉粥样硬化性CVD且未服用他汀类药物的HIV感染成人在基线及3年后测量颈动脉内膜中层厚度。斑块定义为任一部位内膜中层厚度(IMT)>1.5 mm。基线时,中位年龄为43岁(四分位间距,39 - 49岁),85%为男性,74%正在接受抗逆转录病毒药物治疗,50%有斑块。与成人治疗小组III指南相比,美国心脏病学会/美国心脏协会指南更倾向于推荐他汀类药物,总体上(26%对14%;P<0.001)、有斑块者中(32%对17%;P = 0.0002)以及无斑块者中(16%对7%;P = 0.025)均如此。在多变量分析中,年龄较大、低密度脂蛋白胆固醇水平较高、每年吸烟包数以及机会性感染史与基线斑块相关。基线IMT(每增加10%的风险比为1.18;95%置信区间,1.05 - 1.33;P = 0.005)和斑块(风险比为2.06;95%置信区间,1.02 - 4.08;P = 0.037)均与全因死亡率相关,独立于传统CVD风险因素。
尽管与成人治疗小组III指南相比,美国心脏病学会/美国心脏协会指南推荐他汀类药物用于更多HIV感染成人,但两者均未对大多数有颈动脉斑块的HIV感染成人推荐治疗。基线颈动脉粥样硬化而非动脉粥样硬化性CVD风险评分是死亡率的独立预测因素。纳入亚临床动脉粥样硬化检测的HIV特异性指南可能有助于识别动脉粥样硬化性CVD风险增加且可能考虑使用他汀类药物的HIV感染成人。